



Dozens of Case Reports Indicate COVID 'Vaccine'-Induced Turbo Cancer is REAL
So, dear mainstream, you can stop lying and denying the truth.


Remember 2020, when the world was supposedly ravaged by a super-deadly scary evil monster virus from China?
And remember how ‘vaccines’ based on a revolutionary new technology that in fact had a 3-decade history of dismal failure were going to save us from this ‘novel’ virus and its terrifying fatality rate of 0.15%?
The new drugs were hailed as 95% effective, which of course was a lie. In reality, they were 100% effective in obliterating the temporary drop in mortality seen during the COVID sham.
That’s right - excepting places like the UK and US where deliberately inappropriate use of ventilators/medazolam/remdesivir/Do Not Resuscitate orders was especially lethal - mortality in 2020 was actually below the 5-year average.
We all know what happened after that. The ‘life-saving’ pseudo-vaccines were introduced, and excess mortality promptly headed north - to levels not seen since the World War era.
Here are the 2020-2023 mortality figures for Australia:

As you can see from the highlighted row, excess mortality in Australia was below average in 2020. It nudged upwards in 2021 as the vaxxxines were rolled out, jumped like a cane toad in 2022, and remained elevated in 2023.
Now, take a look at the following cause of death figures for the same period.
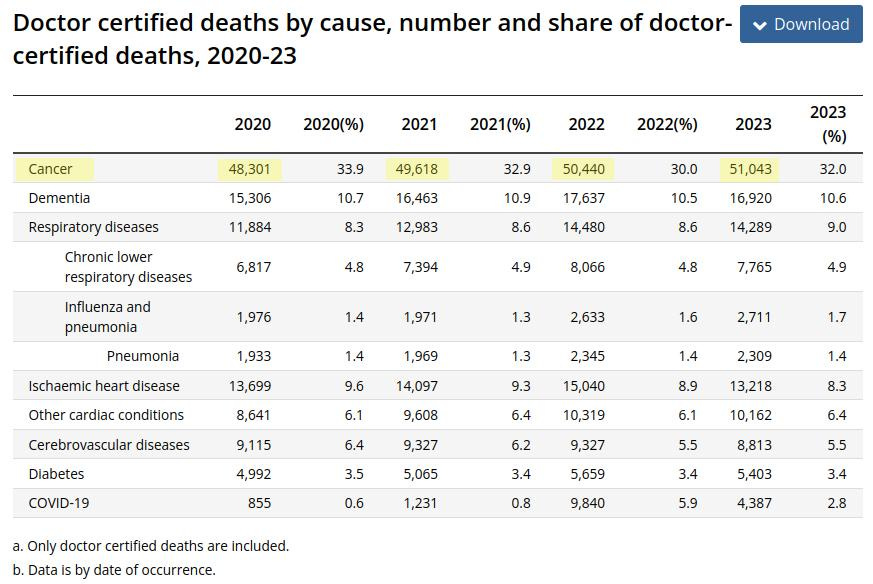
As highlighted, we see a year-on-year increase in cancer deaths between 2020-2023.
All the old excuses like a “growing and ageing population” don’t wash, because deaths from other age-related conditions like ischaemic (coronary) heart disease, stroke, dementia and diabetes actually receded somewhat in 2023.
Because the locals are reproducing below replacement rate, Australia’s post-Covicon population increase has been largely fueled by immigration. Not only do those new arrivals constitute a youngish (working age) demographic, all permanent and provisional visa applicants must have health examinations beforehand to prevent further strain on Australia’s deteriorating health system.
So something out-of-the-ordinary is going on with the cancer death rate.
You’ll also note that, despite the 2023 drop in coronary heart disease deaths, mortality from “Other cardiac conditions” (think myocarditis, pericarditis and ‘sudden’ death) shows a linear increase from 2020 through 2023.
Well, we all know what’s fueling the recent increase in “other cardiac” deaths, but what about cancer?
Roll Up, Roll Up, Get Your Tumors!
After the poison dart rollout, reports of a marked increase in rare and aggressive cancer diagnoses began appearing. Dubbed “turbo cancers”, these malignancies are often already late-stage when diagnosed, increasing the risk of a fatal outcome.
The response of the mainstream - who has egregiously lied to us about everything COVID-related - has been to dismiss the turbo cancer phenomenon as “conspiracy theory”, often insisting there has been no such increase in aggressive cancers.
The problem for the mainstream is that the “turbo cancer” phenomenon wasn’t invented by so-called ‘conspiracy theorists’. There is a similar phenomenon known as “hyperprogressive disease”, and it was identified before the COVID era to describe a sudden acceleration of tumor growth.
What’s more, the wave of sudden tumor growth acceleration that led to the “hyperprogressive disease” definition appeared after medicine introduced a new way of messing with the immune system.
Just like the current turbo cancer phenomenon.
You see, hyperprogession became a recognized phenomenon after immunotherapy was positioned as a preferential treatment for a wide variety of tumors. Unlike the nuke-and-burn approaches of radiotherapy and chemo, immunotherapy drugs are designed to help the immune system recognize and attack cancer cells.
Well, that’s the plan.
The goal is to shrink the tumor, but when oncologists began administering immunotherapy and started noticing tumors grow like they’d never seen before, alarm bells started ringing. At the American Association for Cancer Research Annual Meeting in 2019, a panel of oncologists convened to discuss the concept of hyperprogressive disease - which, some 6 years later, the mainstream media and fact-fudgers are still pretending doesn’t exist.
“There are those who think it's totally illogical that immunotherapy should accelerate tumor growth,” remarked panelist Marina Garassino, MD, from the National Cancer Institute in Milan, Italy. “Then there are others, like myself, who say, ‘I've seen [disease progression] you people wouldn't believe,’ to paraphrase Blade Runner.”
Razelle Kurzrock, MD, of the University of California, San Diego (UCSD), talked about a patient with endometrial stromal sarcoma who, shortly after being given nivolumab, “had an explosive increase of disease in her liver and new, very large tumors in her abdomen.” Another patient with bladder cancer had PET scans that “looked like someone poured gasoline on a fire” less than 2 months following treatment with atezolizumab.
Hyperprogression describes sudden tumor growth in cancer patients; turbo cancer describes the sudden appearance of cancer in previously healthy folks or those who had achieved remission. Both were identified after novel drugs affecting the immune system were introduced. Pre-COVID, the novel drugs were cancer treatments; in 2021, they were gene therapies masquerading as vaccines that would supposedly prevent infection with the non-existent Sars-Cov-2.
At the 2019 ACA meeting, only a minority of the gathered oncologists rejected the immunotherapy-hyperprogression link. Here we are now in 2025, and there is a concerted campaign by the mainstream to deny the turbo cancer phenomenon.
Some oncologists, however, cannot deny what they are seeing with their own eyes - but are unable or unwilling to implicate the vaxxxines.
Instead, they are trying to blame it on ‘inflammation caused by ‘COVID-19’, the re-branded seasonal flu allegedly caused by the non-existent Sars-Cov-2. They are trying to blame COVID, even though “there is no real world evidence connecting COVID-19 to cancer, and some scientists are skeptical about whether there’s an association at all.”
By the way, “inflammation” is not a disease in and of itself but a response to illness or injury. Inflammation doesn’t cause cancer, no more than it causes a sprained ankle.

While some oncologists are refusing to acknowledge the obvious, many others have submitted incriminating case reports that have been published in the peer-reviewed literature.
We’ll take a look at some of those case studies in a moment, but first, let’s see what happened when a group of Japanese researchers correctly pointed out that the vaxxx rollout in Japan was followed by a notable increase in excess mortality and cancer.
Japanese Researchers Report an Increase in Post-Vaxxx Cancers - And Promptly Get Cancelled
In a paper published last year, Gibo et al examined the increase in all-cause and cancer mortality seen after the vaxxxine rollout in Japan, where 80% and 68% of the population had reportedly received their second and third doses, respectively, by March 2023.
They found in 2020 - the first and entirely vaxxx-free year of the pandemic (the Japanese poison prick campaign did not begin until February 17, 2021) - all-cause mortality was below average and there was no excess mortality for all cancers.
Similar to what the official figures show for Australia.
However, in 2021, there was significant excess mortality of 2.1% for all causes and 1.1% for all cancers. In 2022, the excesses increased to 9.6% and 2.1%, respectively.
Another plain fact, again reflecting what was seen in countries like Australia.
Statistically significant excess mortality was observed for three out of 20 types of cancers in 2021, and five out of 20 in 2022. The types were ovarian cancer, leukemia, prostate cancer, lip/oral/pharyngeal cancer, and pancreatic cancer, in descending order in 2022.
Gibo et al had used the 2010-2019 period to determine the baseline predicted mortality rates. A 2023 paper by Scherb and Hayashi used the 2005-2019 period, and similarly found below-average mortality in Japan during 2020, but a crude excess of 8.37% in 2022 (and a 2022 excess of 6.7% in Germany). Scherb and Havashi did not separately examine cancer mortality.
So we have an otherwise unexplained increase in cancer cases that just happened to occur after the mass rollout of toxic drugs based on a technology with a terrible track record. To any non-moron who doesn’t go through life with their head jammed up their keester, that is a highly suspicious sequence of events and demands urgent investigation.
The pharma-owned medicine racket, of course, is in no rush to investigate the potentially malignant drugs they aggressively spruiked with their patently false “Safe & Effective” and “95% efficacy” claims.
Instead, they’re doing what they repeatedly did during COVID whenever some pesky person uttered an inconvenient truth:
Calling them names and shutting them down.
Which is a sure sign they’ve got something to hide.
When a Study Finds Something Inconvenient, Have it Retracted
In the world of medical journals, an article retraction used to be a big deal. This was when an article made it through the peer-review process, then was later found to have been fraudulent or possessed serious methodological flaws that somehow escaped the peer-reviewers’ attention. The journal would then issue a solemn retraction notice.
During the scamdemic, however, retraction notices became a regular occurrence, skyrocketing in number. Lo and behold, the newfound excess of retracted articles almost always happened to be those that didn’t support the mainstream COVID narrative.
The authors of a retracted article deserve an explanation by the journal as to what they allegedly did wrong, but the retraction notices issued during the scamdemic invariably contained no details, just vague statements claiming the journal had been made aware of “concerns” about the “methodology” of the study.
It was akin to accusing a person of a crime because someone, somewhere, said they didn’t like the way that person looked.
And so, two months after Gibo et al published their findings, the journal Cureus issued an Expression of Concern, claiming “The Editors-in-Chief have been made aware of several concerns regarding the scientific credibility of this article. A comprehensive post-publication editorial review is being conducted to determine if any action is required.”
In other words, the usual vague, non-committal textbook classic waffle that indicated they’d been tapped on the shoulder and told, “oi, you can’t be publishing this stuff.”
Two weeks after their so-called Expression of Concern, the Cureus editors issued a Retraction Notice. The limp-dicked statement read:
“The Editors-in-Chief have retracted this article. Upon post-publication review, it has been determined that the correlation between mortality rates and vaccination status cannot be proven with the data presented in this article. As this invalidates the conclusions of the article, the decision has been made to retract.”
Looks to me like corruption and cowardice - two of the world’s primary driving forces - had won yet again.
Cureus added:
“The authors disagree with this retraction.”
Of course the authors disagreed with the retraction, because it was complete garbage. At no point in their paper did Gibo et al claim their analysis had “proven” anything.
Here is exactly what they stated in their conclusion:
“Statistically significant increases in age-adjusted mortality rates of all cancer and some specific types of cancer, namely, ovarian cancer, leukemia, prostate, lip/oral/pharyngeal, pancreatic, and breast cancers, were observed in 2022 after two-thirds of the Japanese population had received the third or later dose of SARS-CoV-2 mRNA-LNP vaccine. These particularly marked increases in mortality rates of these ERα-sensitive cancers may be attributable to several mechanisms of the mRNA-LNP vaccination rather than COVID-19 infection itself or reduced cancer care due to the lockdown. The significance of this possibility warrants further studies.” (Bold emphasis added)
Clearly, the editors of Cureus were being disingenuous. Because at no point do Gibo et al claim the compelling correlation they observed equaled causation. The epidemiological data, derived from Japan’s tightly kept public health records, do indeed warrant further investigation, as do the documented case studies of people with unremarkable health histories who suddenly developed malignancies after getting injected with toxic drugs made by corporate criminals.
So don’t hold your breath waiting for authorities to admit the vaxxxine-cancer link. You’ll end up deader than a hateful journalist who celebrates getting vaxxxed on social media.
The Case Studies They Don’t Want You to See
While the mainstream media and fact-fudgers are vigorously downplaying a link between the aggressive vaxxxination rollout and a surge in aggressive, late-stage cancers, dozens of incriminating case reports are accumulating in the medical literature.
These reports often feature patients with no known health issues, who suddenly developed malignancies shortly after receiving the COVID ‘vaccines’. Others feature patients who had previously recovered from cancer, only to relapse after having a shot or two of the Kovid Kool-Aid.
Below is a list of case reports I have retrieved via a cursory Internet search; it is by no means an exhaustive list and I’m sure a more extensive search would retrieve further citations.
It’s a lengthy list, so if you are time poor or have an abbreviated attention span, you may want to scroll to the cases in which the known outcome was fatal. Those alone should convince you the link between vaxxxination and cancer needs urgent attention. Those cases in which the known outcome was lethal have been prefixed with **.
Case Studies of Patients Who Developed Cancer Shortly After Receiving ‘Vaccines’ Based on Failed Technology
Let’s start with **Hetta et al 2025, a recent case report from the UK that helps demonstrate what a truly Frankensteinian class of drugs we are dealing with.
The patients in this case report suffered ultimately fatal primary tumors of the heart after being vaxxxinated. Primary cardiac tumors are normally very rare, with an incidence of approximately 0.02% - corresponding to 2 tumors in 10,000 autopsies. Around 25% of these are malignant. The prognosis for these types of tumors is poor.
Case 1 involved a 49-year-old Black African male presenting with chest pain and breathlessness 4 weeks after his first Pfizer shot. Initially treated for pericarditis, he returned with worsening symptoms. Imaging confirmed a right atrial mass diagnosed as malignant. The patient developed atrial fibrillation likely due to compression from the tumor, as well as renal complications and severe anemia. He died 4 months after diagnosis.
Case 2 was a 43-year-old Caucasian male with asthma and recent COVID-19 ‘vaccination’ (the brand of poison was not mentioned) who presented with a 3-week history of cough and breathlessness. Initially treated for pneumonia, his symptoms persisted despite antibiotics.
At 10 months, imaging identified a large posterior pericardial mass. The highly vascular, myocardium-invading tumor made surgical removal unfeasible, so the patient instead received six cycles of chemotherapy. This resulted in some improvement and minor tumor reduction, however the patient succumbed to his illness 24 months after initial presentation.
**Schwartzenberg et al 2023 reports on a particularly disturbing case that only the most shameless vaxxx shills would dismiss as ‘coincidence’. It occurred in Israel, the “test case” country where Albert “The Criminal” Bourla is adored while innocent Palestinian children are deemed such a threat they are blown off the planet.
A previously healthy 22-year-old man, with no history of smoking or asbestos exposure, presented with chest pain and shortness of breath. A month earlier, he’d received his second dose of the Pfizer vaxxx.
Acute pericarditis was diagnosed, which initiated a recurrent cycle of admission/discharge, treatment with ibuprofen/prednisone/colchicine, and pericardial drainage.
Four months after initial presentation, chest X-ray revealed heart enlargement and a new CT study revealed pericardial thickening. Further investigation revealed “the entire heart and the great vessels were wrapped by a severely inflamed 3 cm thickness of fibro-gelatinous layer”.
Thanks to the Bibi and Bourla collab, this youngster had been given a one-way ticket to Destination F@#ked. His heart was effectively being strangled, and there was little the doctors could do. He developed multi-organ failure and died 3 weeks later.
I believe this is the bit where the hopelessly brainwashed retort, “At least he was vaccinated, or it could’ve been much worse!”
This is an article about turbo cancer, so obviously there’s more to the story. After the young patient died, examination of a specimen taken from his heart led to a diagnosis of pericardial malignant mesothelioma.
The authors wrote:
“To the best of our knowledge, this is the only second case of pathologically confirmed pericarditis that transformed into mesothelioma, in this case within only 4 months. It is unlikely that an earlier correct diagnosis would have made a clinical difference in this case in view of the accelerated disease course.”
**Ueda et al 2024 reported on a 61-year-old woman with systemic lupus erythematosus, presenting to hospital with impaired consciousness, fever, muscle spasms and left-side paralysis. One month prior, she received her second dose of the Pfizer vaxxxine. She was diagnosed with hemophagocytic lymphohistiocytosis, a serious condition where the immune system goes into hyper-drive and attacks the body instead of foreign entities. A rare condition in adults, HLH normally strikes infants and children.
Despite treatment, the patient died on day 75. An autopsy was performed and the presence of intravascular large B-cell lymphoma was confirmed.
Noting the pattern of disease development, the researchers said “we speculate that the COVID-19 vaccination and her autoimmune condition may have expedited IVLBCL development.”
As it turns out, lymphomas (cancers of the lymphatic system) and leukemias (blood-related malignancies) are common themes in case studies of post-vaxxx cancer.
Goldman et al 2021 reported on a 66-year-old man with no significant medical history except for hypertension and diabetes who presented with cervical lymphadenopathies. He’d received two doses of the Pfizer vaxxx 5 and 6 months earlier.
A PET-CT scan led to a diagnosis of angioimmunoblastic T cell lymphoma. In one of those decisions that makes you shake your head in wonder, fourteen days after the scan the patient was given a “booster” dose of the Pfizer vaxxx “in preparation of the first cycle of chemotherapy.”
You know, kind of like how you spray gasoline all over a raging fire in preparation for the first arrival of the fire department.
After the booster dose, the malignancy did indeed go into boost mode. Within a few days, the patient reported noticeable swelling of right cervical lymph nodes. A second PET-CT was performed 8 days after the booster shot, and it revealed the cancer had broken out like a prison riot.
The scan "demonstrated a clear increase in number, size and metabolic activity of pre-existing lymphadenopathies ... Furthermore, new hypermetabolic lymphadenopathies and new hypermetabolic sites had developed since the first examination, in several different locations ... there was a marked 5.3-fold increase in whole-body TLG (total lesion glycolysis index)".
For those not schooled in oncologyspeak, the plain English translation is:
"What the #@$%?!"
At the time of the case report (2 weeks after start of treatment with such fun drugs as methylprednisolone, brentuximab, vendotin, cyclophosphamide and doxorubicin), the lymph node swelling had decreased, and “the overall performance status of the patient is improving.”
Zamfir et al 2022 gushes about what “outstanding achievements” the vaxxxines were, then describes two cases of lymphoma diagnosed shortly after the administration of the Pfizer vaxxx. One patient was a female who’d received two doses, the other a male whose symptoms appeared within days of his initial shot. Both patients were being treated for their malignancies at the time the case report was filed.
Khatri et al 2024 described the case of a 60-year-old Asian female who received her first dose of the Pfizer vaxxx in August 2021. Right after her vaccination, she developed lymph node swelling in her right armpit. After her second vaccine dose in September 2021, she developed lymph node enlargement in her neck and groin. Further investigation led to a diagnosis of diagnosis of angioimmunoblastic T-cell lymphoma. She received 6 cycles of chemotherapy and was in remission at the time of the case report.
Veeraballi et al 2022 describes a 74-year-old female who presented to the emergency department with shortness of breath and generalized weakness for two days. The symptoms began after receiving her first dose of the Johnson & Johnson vaxxxine.
She was diagnosed with concomitant chronic myelomonocytic leukemia and scleroderma. As the researchers noted, this is normally a very rare combination and “suggests the possibility of developing CMML after receiving the J&J COVID vaccine.”
It also strongly suggests you should never take anything made by a company whose claims to fame include knowingly selling asbestos-laced baby powder for decades on end.
Tachita et al 2023 report on a 73-year-old Japanese male presenting with a lump in the left arm, where he received the Pfizer vaxxx 3 months prior. Despite treatment with topical corticosteroids and debridement (removal of dead/damaged/infected tissue), the tumor progressed. Additionally, fever, night sweats, and general fatigue were observed.
Further examination led to a diagnosis of extranodal NK/T‑cell lymphoma.
The patient had a history of myocardial infarction and a cardiac aneurysm, so repeated cycles of reduced-dose chemotherapy were employed to avoid cardiac complications. A partial response, in the form of tumor regression was seen, before chemo was terminated due to toxicity. Radiotherapy was then employed to target the remaining lesion.
Ukishima et al 2022 reports a 45-year-old man with no specific medical history, who got his third Moderna shot and promptly developed a fever that wouldn’t go away. After 5 weeks of this, he sought medical help.
Physical examination revealed a rash in and around the patient’s belly button, accompanied by pain and warmth. The rash appeared 3 weeks after the third Moderna shot.
Further investigation led to a diagnosis of subcutaneous panniculitis-like T-cell lymphoma. This type of T-cell lymphoma is rare with a relatively good prognosis, although recurrence is frequent.
The patient received chemotherapy and prednisone. After 3 months of follow-up, his skin changes and other symptoms had abated.
Yanagida et al 2023 described a A 55-year-old man presenting with an enlarged bilateral neck lymph node that he noticed two days after his first dose of COVID mRNA vaxxxination (brand not specified).
A diagnosis of natural killer-lymphoblastic leukemia/lymphoma ensued, followed by chemotherapy and bone marrow transplantation.
Cavanna et al 2023 describes a a 66-year-old Italian man with no previous health history who presented with a lymphadenopathy around 10 days after receiving his third dose of the Pfizer vaxxx. Further enlargement and the appearance of another lymphadenopathy over the next 3 months prompted further investigation, which led to a diagnosis of stage-II non-Hodgkin lymphoma. After six cycles of chemotherapy the patient was “well and in complete remission.”
Their experience with this patient led the researchers to perform a search of the literature for similar cases. They retrieved five other papers (Kreher 2022; Sekizawa 2022; Revenga-Porcel 2023; Mizutani 2022; Tang 2022; Zamfir 2022 - discussed above) reporting on 8 individual patients, 5 of whom were diagnosed with B-cell lymphoma. Their lymphadenopathies became evident 1-10 days after receiving a vaxxx dose; in 6 of the cases, this occurred after the first dose. Five patients had been pricked with Pfizer, one with AstraZeneca, one with Moderna, and another with Janssen (a subsidiary of Johnson & Johnson).
Bizarrely, the researchers wrote:
“We are aware that the link between COVID-19 vaccination and lymphoma most likely is a chance phenomenon, and that COVID-19 vaccines represent very efficient products for many people around the world. However, we believe that clinical events, even if only temporally associated with novel treatments or novel vaccines, should be reported for the benefit of the patients and the scientific community”
Here’s what they are really trying to say, but can’t:
“We know damn well this phenomenon can’t be dismissed as pure coincidence, but if we said that our livelihoods would be in serious jeopardy. We want to alert people to the dangers, but without being reprimanded or fired. So forgive our evasive wordcraft and read between the lines, okay?”
Olszewska et al 2024 reviewed 12 case study papers (Brumfiel 2021; Panou 2022; Koumaki 2022; Li 2022; Kreher 2022; Hobayan 2023; Zamfir 2022; Revenga-Porcel 2023; Bresler 2023; Hooper 2022; Montoya 2022; Avallone 2023), encompassing 24 individual patients who were diagnosed with primary cutaneous lymphomas following COVID ‘vaccination’.
Most were T-cell lymphomas (67%), appeared after receipt of the mRNA-based vaccines (79%), and predominantly after the first dose (54%). The cases exhibited a tendency to worsen following subsequent COVID-19 vaccinations. Outcome was not mentioned in a number of studies, most others reported a favorable outcome after treatment.
Erdoğdu et al 2022 reported on five cases of blood-related disorders after administration of the Pfizer vaxxx, 3 of which proved to be malignant.
The first involved a 49-year-old female who, two days after receiving a Pfizer shot, experienced increasing weakness and fatigue. Hospital admission ten days later led to a diagnosis of B-cell acute lymphoblastic leukemia and the initiation of chemotherapy.
Acute lymphoblastic leukemia is a rare white blood cell cancer with a poor prognosis. The 5-year overall survival is only 35% in patients aged between 18 to 60 years.
The second patient was a 47-year-old female, who had previously received extensive treatment for B-cell lymphoma 2 years previously. After fourteen months in remission, she reported dyspnea and fatigue after receipt of the Pfizer shot. A diagnosis of acute lymphoblastic leukemia ensued, and treatment commenced in the intensive care unit, which was continuing at the time of the case report.
The last case was a 67-year-old female patient previously diagnosed with acute myeloid leukemia in 2007, for which she had been treated and from which she remained in remission for 14 years. However, in July 2021, she received two doses of “inactivated SARS-CoV-2 vaccine” (not named, but presumably the Chinese Sinopharma and/or Sinovac drugs). In September 2021, she further received the Pfizer shot and experienced fatigue and weakness afterwards. Acute myeloid leukemia was diagnosed and treatment was initiated.
In Cinar et al 2022, the same group of Turkish researchers presented another four case reports of individuals who developed acute myeloid leukemia soon after their most recent vaxxxine shot. The youngest was an an otherwise healthy 28-year-old female who had received 2 shots of the Pfizer drug, the oldest was a 72‐year‐old man with a history of diabetes, hypertension, and coronary artery disease who’d received his fifth dose of the Pfizer vaxxx approximately five weeks before the complaints emerged.
Ang et al 2023 reported on an otherwise healthy 43-year-old female patient in Taiwan who received a booster dose of the Moderna vaxxxine on January 3, 2023. A day after this injection, she felt ill with dizziness, mild dyspnea, and general malaise.
Prior to her most recent Moderna shot, the patient had already received four COVID-19 ‘vaccinations’, including two doses of the AstraZeneca clot shot, a “half-dose” of Moderna, and a dose of the “protein subunit” NovaVax, all between June 2021 and July 2022.
Subsequent examination led to a diagnosis of acute lymphoblastic leukemia.
Bae et al 2023 reported on a 73-year-old female with a past medical history of hypertension, hyperlipidemia, and surgery for a benign kidney tumor. She presented with worsening right upper arm swelling, which began two to four days after receiving her second dose of the Moderna vaxxxine. MRI revealed a 5.2 cm soft tissue mass overlying the triceps region, further examination of which led to a diagnosis of high-grade sarcoma (sarcomas are cancers that start in connective tissues such as bone, cartilage, muscle, fat, or vascular tissues). The mass was surgically removed (resected) four months after the initial visit.

**Asif et al 2023 describes a 26-year-old woman with no pertinent medical history who presented to the ED with lumps in her left groin 5 days after receiving a second Moderna shot. On physical examination, lymphadenopathy was noted and suspected to be a reaction to her recent shot. Follow-up with her primary care provider was advised; the problem not only persisted but worsened.
An initial diagnosis of metastatic melanoma was followed by a rapid decline in her condition and the initiation of immunotherapy. Additional testing of biopsy samples led to an updated diagnosis of clear cell sarcoma, a very rare form of soft tissue sarcoma.
The decision was made to continue with immunotherapy. However, the patient developed acute renal failure accompanied by worsening encephalopathy. The patient and her family elected to proceed with comfort measures, and she died later the same day.
**Kyriakopoulos et al 2023 reported on a 56-year-old white male with no health conditions, and whose family history of malignancy consisted of his mother suffering lung cancer due to smoking. He presented with “a massive and aggressively infiltrating basaloid-featured cancer in the right side of his face that rapidly evolved, ultimately ending in the patient’s death.”
The symptoms began four days after his first Pfizer vaxxxine shot, when he presented with severe pain in his RHS temple area, spreading to the temporomandibular (jaw) joint. The pain continued unabated and even worsened over the following two months despite use of anti-inflammatories, so the patient underwent a brain MRI examination.
This led to an initial diagnosis of of Bell’s palsy, a common side effect induced by the vaxxxines.
His condition worsened, so he was treated with “intravenous vitamin C, plus oral vitamin D, quercetin, melatonin, zeolite and, after a week, reported dramatic improvement in pain and weakness symptoms.”
Sadly, the improvement was transient. The patient suffered progressive wasting and weight loss (12 kg) with progressing facial palsy symptoms. Around eight months after his Pfizer injection, CT brain scan revealed a diffuse tumor of the right parotid (salivary) gland. Because the peripheral margins of the tumor were not clear, surgical excision of the tumor was not considered viable and the patient’s only treatment was palliative morphine administration. The patient passed away 4 months after the biopsy.
The paper features numerous photos of the patient prior to his passing; I won’t re-post them here because some are quite graphic. However, if you know someone who thinks the turbo cancer phenomenon cancer is a “conspiracy theory”, those photos might help snap them out of their stupor. Or maybe not - the river of denial runs pretty deep in some vaxxxine believers.
The researchers note their case report was hampered by “the refusal of the hospital that performed the biopsy to provide the histopathological images or perform immunohistochemical staining for the spike protein.”
While compiling the case report, the authors searched VAERS and found a total of 192 cases in which vaccines were linked to metastasis in 2021; 189 (98.4%) of those reports involved COVID vaxxxines.
Another interesting aspect of this paper is that one of the authors was Peter McCullough, who despite the mountain of incriminating evidence he has been privy to, has praised the disastrous mRNA technology and even proposed more dodgey gene therapies to counter the ill-effects of this currently available gene therapy.
Martínez-Ortega et al 2024 describes the case of a 73-year-old man with no other health conditions who presented to a dermatology clinic in Guadalajara, Mexico with some nasty-looking lesions and nodules on the back of his right hand. He reported the condition appeared one week after receiving the third dose of the AstraZeneca vaxxxine, gradually growing over the course of two months and ultimately leading to the development of a tumor. Cryotherapy was selected as the treatment approach, achieving full clearance of the lesions after three sessions, each spaced three weeks apart.
Hitzenbichler et al 2024 reported on a 48-year-old German male previously and successfully treated for Kaposi’s sarcoma on his right foot sole and lower leg in 2008. In June 2021, a week after receiving a second dose of the Moderna vaxxxine, he noticed lesions on the sole of his right foot. In December 2021, he received a “booster” shot of the Pfizer vaxxxine. A week later, one of the lesions on his sole progressed to an ulcerative tumor. He presented at the local sarcoma center where the tumor was resected. Histology confirmed Kaposi’s sarcoma.
Yilmaz et al 2024 report a case of primary cutaneous adenoid cystic carcinoma localized in the patient’s subcutaneous tissue of the scapular region, that grew after receipt of the Pfizer vaxxx.
Yumeen et al 2023 report on a 66-year-old male presenting with a painful, solitary skin lesion on his right shoulder. Within a week of receiving of the Moderna vaxxx, he noted development of the lesion in exactly the same location where he had been injected. The patient had a past medical history of osteoarthritis, but no other chronic medical conditions, no allergies, nor any prior history of skin disease.
Further examination confirmed the lesion was a keratoacanthoma, a type of skin cancer that starts as a small, pimple-like lesion and typically develops into a dome-shaped, skin-colored nodule with a central depression filled with keratin (the major protein found in hair, skin, and nails).
The lesion was successfully removed via surgery.
The authors had no doubt as to what caused the lesion. “It is important for both physicians and patients to be aware of adverse cutaneous reactions that can occur following COVID-19 vaccination,” they noted, “so that these can be appropriately diagnosed and managed.”
White et al 2023 reported on a 75-year-old Egyptian woman suffering redness, irritation, and what she described as “bubbling” in her right eye. The patient had a history of ocular disorders, and used eye drops to treat her glaucoma and dry eyes.
The symptoms she sought help for developed a few weeks following her Pfizer ‘booster’ shot. Investigation led to the diagnosis of Kaposi sarcoma. Treatment with interferon was unsuccessful, so radiation therapy was then employed. This resulted in “a marked decrease” in the size and vascularity of the lesions, with a slow improvement in her appearance over the following three months.
Nishizawa et al 2023 describe a 42-year-old male with no remarkable medical history who experienced swelling of his left armpit lymph node a week after his third vaxxx shot (brand not mentioned). He initially brushed it off as a a routine reaction to the shot, but the mass grew rapidly over the next few months.
A biopsy performed after he presented to hospital revealed metastatic melanoma.
Within a month of the initial visit, his condition had turned life-threatening. Not only had the armpit mass grown further, but systemic edema, dyspnea, hypertension, tachycardia and congestive heart failure were also observed.
Immunotherapy using nivolumab plus ipilimumab was begun, along with diuretics and antihypertensive drugs for his heart failure. The tumor shrank significantly after the first three courses of the therapy, but after after the fourth course, the tumor began growing again. In addition, the heart failure flared, and new mediastinal lymph node metastases appeared.
Treatment was switched to encorafenib/vinimetinib. The tumor shrank markedly and the heart failure improved after one month. At month 4 of this treatment, the patient achieved complete remission. Below is a visual timeline of the patient’s progress.

Wolfson and Kim 2023 describes a 60-year-old woman with no personal or family history of breast cancer who presented for routine screening mammography. Nine weeks earlier, she had received a second dose of the Moderna vaxxx in her left arm.
The mammography showed a new mass in the left breast, and a new dense lymph node in the left armpit area. Pathologic examination of the breast mass and lymph node confirmed carcinoma. The patient subsequently underwent chemotherapy followed by breast-conserving surgery and radiation therapy.
Tripathy et al 2022 reported the case of a 61-year-old Caucasian female who had been diagnosed with lung and lymph node carcinomas in 2017. After extensive immunotherapy, she achieved a partial response and remained stable over the next four years.
At the recommendation of her oncologist and following guidelines of the hopelessly corrupt CDC, the patient received the Pfizer vaxxx in March 2021. Two weeks following her vaccination, she developed a palpable lymph node behind her left ear. Biopsy confirmed tumor recurrence with an aggressive form of cancer known as poorly differentiated carcinoma. Chemotherapy was initiated, again achieving a partial response.
Aimo et al 2022 describes a 45 year old woman with a history of alcohol and drug abuse, fatty liver, hiatal hernia, and anxious–depressive syndrome. She presented to hospital complaining of muscle weakness and skin rash/scarring.
Investigation led to a diagnosis of breast cancer and paraneoplastic dermatomyositis. When asked, the patient that ten days earlier she had received the AstraZeneca vaxxx.
Treatment with steroids and immunoglobulins ensued, followed by a right mastectomy. Her condition improved and she was eventually discharged from hospital.
Bharathidasan et al 2023 describes the case of a 70-year-old Hispanic male who presented to an urgent care clinic with abdominal pain, nausea, headache, myalgia, and severe constipation. The day prior, he received his fourth dose of COVID vaxxx (brand not stated). He was asymptomatic prior to receiving the injection, had completed all age-appropriate cancer screenings, and his only past medical history was well-controlled benign essential hypertension.
Abdominal x-ray showed no obvious issues, so the patient was reassured he was experiencing expected side effects of the vaccine and was sent home. He returned to the ED two days later complaining of a right-sided neck swelling that had been increasing in size since the day of his vaxxxination. Further investigation led to a finding of prostate cancer, which was treated with anti-androgens.
Summary
The above article encompasses over 40 case report papers, some involving multiple patients, who evinced new, and in some cases recurring, malignancies after receiving the Pfizer, Moderna, AstraZeneca, J&J/Janssen and Chinese vaxxxines.
Many of the case reports involved people with unremarkable health histories.
To dismiss all these cases as mere coincidence, and to persist with the claim that vaxxx-induced turbo cancer is a baseless conspiracy theory, is a glaring admission of either monumental stupidity, terminal dishonesty, or direct involvement in the monumental fraud that is COVID and its associated ‘vaccination’.
Addendum: The following case studies of benign pituitary tumors are noteworthy.
Aliberti et al 2022 describe a 50-year-old man presented to emergency with severe headache, vomit, nausea and diplopia that started after his third vaxxx shot (Moderna). The patient did not smoke, did not take any pharmaceuticals, and reported kidney stones 15 years earlier.
Examination revealed a pituitary macroadenoma that had hemorrhaged, a condition known as pituitary apoplexy. Pituitary macroadenomas are usually benign, but when they hemorrhage the patient needs to get to an ED pronto. That, and the fact there have been numerous case reports of pituitary apoplexy subsequent to COVID vaxxxination, warrants further discussion.
In this case, emergency treatment was followed by removal of the tumor, and medication until adrenal function returned to normal. At 4 months follow-up, the patient had normalized and was undergoing periodic follow-up.
The authors filed a Vaccine Adverse Drug Reaction report to the Italian Medicines Agency. They also searched the literature for other cases of post-vaxxx pituitary apoplexy, and found reports by Piñar-Gutiérrez 2021; Jaggi 2021; Roncati 2022, and; Zainordin 2022. Three of the cases involved the AstraZeneca vaxxx, in Jaggi 2021, the vaxxx brand was not stated.
Srimanan & Panyakorn 2023 describes a 60-year-old Thai woman who experienced vision loss in her left eye five days after her fourth dose of the Pfizer pfilth. Neuroimaging revealed a benign pituitary tumour that was compressing her optic nerves. Tumor removal was successfully performed and her vision significantly improved.
The authors described this as “an interesting case that supports the COVID-19 vaccine as one of the possible risk factors aggravating [pituitary adenomas]”.
Wow...
It's stunning to consider the COVID-19 injections were mandatory in Australia, with people under threat of losing their livelihood and participation in society if they refused to submit to the mandated medical interventions.
The vaccinators collaborated with this travesty, violating their own personal obligation to obtain valid voluntary informed consent for vaccination.
For more detail, see:
- The Australian Government destroyed valid consent for COVID-19 vaccination... https://elizabethhart.substack.com/p/the-australian-government-destroyed
- Mafia with a needle... https://elizabethhart.substack.com/p/mafia-with-a-needle
Brother-in-law, brain cancer, detected May 2021, passed away June 2021. Ex-wife, leukemia, detected fall 2021, 40+ transfusions & chemo treatments later, still here. Friend who I worked on the RFK Jr. campaign with (& was coerced by his job) just diagnosed w/pancreatic cancer, prognosis not good. Business associate also just diagnosed w/prostate cancer. All jabbed by mRNA. If this is just my little world, what does that mean for all of humanity?