



Pfizer-BioNTech COVID-19 Vaccine: The 'Life-Saving' Drug that Seems to be Killing People
Today we're going to discuss some of the less-publicized facts about the absurdly-hyped Pfizer-BioNTech vaccine, the first of the COVID-19 vaccines to be granted widespread "emergency use authorization" in the West. All around the world, people are mysteriously dying shortly after receiving the vaccine. And it's not just "frail" elderly folks who are dying after getting injected, but also younger and healthy folks.
Code-named BNT162b2, and sold under the brand name Comirnaty, the vaccine was developed by German biotech company BioNTech in cooperation with the multinational drug giant Pfizer.
In order to allow Comirnaty to market, the usual drug approval process and its accompanying scrutiny were tossed to the wind as regulators around the world rushed to award the drug "emergency use" status. This meant the Pfizer-BioNTech vaccine could be prematurely unleashed on an unsuspecting public in order to save the world from the largely asymptomatic coronavirus whose infection fatality rate is measured in fractions of a percent.
On 7 December 2020, the United Kingdom became the first country to authorize the vaccine's use on an emergency basis. Other countries promptly followed, including Canada, Bahrain and Saudi Arabia, Mexico, Chile, Panama, Costa Rica and, of course, the US, where the Food and Drug Administration (FDA) authorized Cominarty for emergency use on Friday, 11 December 2020.
And on Tuesday, 31 December 2020, the World Health Organisation (WHO) listed the vaccine as part of its Emergency Use Listing (EUL). This made the Pfizer/BioNTech vaccine the first COVID vaccine to receive emergency validation from the WHO.
What has been lost among this rush of "emergency use" approvals, and repeated assurances the drug is "safe and effective," is the fact that clinical testing of the vaccine is not yet complete. The requisite Phase III clinical testing, which kicked off on 29 April 2020, is still ongoing. The estimated completion date for primary outcomes is 30 July 2021, while monitoring of secondary outcomes is set to continue until 27 January 2023. Under normal circumstances, satisfactory completion of Phase III clinical trials is a prerequisite for gaining drug approval. That's why the drug required the loophole of 'emergency use' authorization to get to market so quickly - despite all disingenuous claims to the contrary, the drug has not been fully tested.
This does not bode well for public health, because even drugs that go through the full approval process have a high likelihood of producing serious side effects. Researchers from Yale School of Medicine found nearly a third of drugs approved by the FDA from 2001 through 2010 had major safety issues years after the medications were made widely available. Seventy-one of the 222 drugs approved during the decade were withdrawn, required a "black box" warning on side effects or warranted a safety announcement about new risks. It took a median of 4.2 years after the drugs were approved for these safety concerns to come to light, the study found, and issues were more common among psychiatric drugs, drugs approved near the regulatory deadline for approval, biologic drugs and drugs that were granted "accelerated approval."
There's another wee problem with Comirnaty (and many of the other COVID vaccines being rushed to market). Not only is the Phase III testing incomplete, but the Pfizer-BioNTech COVID-19 vaccine uses technology that is relatively new and unproven, and therefore of unknown safety and efficacy.
To understand why the new mRNA vaccines are so different, a quick explanation of current vaccines is in order.
Most influenza vaccines are made by growing weakened forms of the target virus using chicken eggs. Fluid containing the virus is then harvested from the eggs, purified, filled into vials (often along with other highly questionable ingredients such as thimerosal a.k.a. ethyl-mercury), then shipped off to be injected into the unquestioning masses, who receive a "dead" (inactivated) form of the virus. This is the most commonly-used method and has been employed for over 70 years.
More recent additions to the flu vaccine arsenal include:
-Nasal spray flu vaccine (FluMist), which contains a live but weakened virus;
-Vaccines produced using cultured mammalian cells instead of eggs;
-Recombinant vaccines, made by combining DNA for making hemagglutinin (a surface protein and antigen found on influenza viruses) with a baculovirus, a virus that infects invertebrates. The resultant “recombinant” virus is introduced into host cell lines, which are instructed by the hybrid virus to produce the antigen. This antigen is grown in bulk, collected, purified, and then sold as recombinant flu vaccine.
The premise behind vaccines is that your immune system has white blood cells that recognize unwanted intruders by their antigens. By giving someone a vaccine containing antigens for a virus, your B lymphocyte cells can start making antibodies. If that person is later infected with that virus, the antibodies already present will attach to the pathogen and tag it for termination.
And Now, Welcome to the Brave New World of COVID Vaccines
So that's a very brief rundown of what the world of flu vaccines looked like prior to COVID-19. But as the world collectively shat its panties over a virus with an infection fatality rate of less than 0.5%, a bunch of technocratic billionaires and their politician friends decided we needed a new vaccine and yesterday, damnit!
They picked up the phone and called their buddies at Big Pharma, and gave them the brief. They told them time was of the essence. There was huge money to be made, uh, I mean, lots of lives to be saved, but they had to strike while the iron was hot, uh, I mean, before the virus mutated into COVID-21 or DAVID-22 or ROCCO-Z28 or some other stupid vanity plate-named pandemic.
And this is where the COVID story takes another interesting turn. While Astra Zeneca - a corporate criminal, just like Pfizer - went with a traditional vaccine approach, companies like the latter and Moderna opted for a more high-tech approach.
The latter made the decision to run with a once-dismissed technology involving synthetic messenger RNA (mRNA). The typical government/mainstream media explanation of these new mRNA vaccines is that "they teach our cells how to make a protein ... that triggers an immune response inside our bodies. That immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies."
And so, in the official rosy-cheeked version of events, mRNA vaccines are like dear old Mrs Appleton, your sweet first-grade teacher who taught you to count to ten and tell the difference between the letters "C" and "K", even though they often sounded the same. Or was that Big Bird on Sesame Street? Anyways, you get my point ... mRNA vaccines are being made to look as helpful, benevolent and non-threatening as possible.
But based on what has emerged so far, mRNA vaccines are looking a lot less like Mrs Appleton and a lot more like Myra Hindley. Except deadlier.
A Brief History of mRNA Technology
To be sure, the mRNA story sounds great on paper. The kind of paper that comprises a company prospectus. The body uses mRNA to instruct cells which proteins to make, so, in theory, if you could design your own mRNA, you could manipulate the process and create proteins to vaccinate against infection, reverse rare diseases, or repair damaged heart tissue.
The early pioneer of mRNA technology was Hungarian-born scientist Katalin Karikó. According to various media stories, her early belief in the potential of mRNA to fight disease was not shared by governments, corporate funders, and even many of her own colleagues. Her mRNA quest proved something of a career dead end as she struggled with rejections and demotions. Well, at least until COVID-19 became a thing.
The stumbling block was that injecting synthetic mRNA often backfired and caused an unwanted immune response; the body sensed a foreign intruder and went into attack mode. Turns out one of the RNA nucleosides in its altered, synthetic form was throwing everything off by triggering the immune system. So Karikó and her Penn State colleague Drew Weissman swapped it out for a slightly modified version, creating a hybrid mRNA that could seemingly sneak its way into cells without alerting the body’s defenses. Well, under experimental lab conditions, at least.
This discovery was first published in 2005 and while it largely flew under the radar, according to STAT+ it did catch the attention of one Derrick Rossi, who would later help found Moderna. Rossi and his partners started Moderna in 2010, but internal squabbling saw him leave the company in 2014. The mRNA concept he introduced to his partners, however, stayed behind.
Under its "brash" and entrepreneurial CEO, Stéphane Bancel, Moderna went on to raise billions of dollars, going public in 2018. Its promise to investors relied on a range of mRNA medicines that could be safely dosed over and over. But behind the scenes, reports STAT+, the company’s scientists were running into a familiar problem. In animal studies, the ideal dose of their leading mRNA drug was triggering dangerous immune reactions — the kind for which Karikó had seemingly improvised a workaround — but a lower dose had proved too weak to show any benefits. If repeated doses of mRNA were too toxic to test in human beings, the company would have to rely on something requiring only one or two injections to show an effect. And so Moderna put its stable of experimental drugs on the backburner and morphed into a vaccines company. It's worth noting that, despite the numerous drugs it has researched, prior to COVID-mania Moderna had yet to create a drug that achieved regulatory approval.
It was a similar story at BioNTech. Despite going public in October 2019 and closing with a market value of $3.4 billion, and having 13 compounds in clinical trials for a variety of ailments, prior to COVIDiocy BioNTech was yet to get a product approved. When the COVID-19 panic took hold and cries for a vaccine intensified, BioNTech saw a golden opportunity. The company knew it could benefit from the clout of Big Drug, and so asked Pfizer if it would be interested in a partnership. The answer was a resounding yes, not suprising given the financial windfall - the US federal government agreed to pay the two companies almost $2 billion for at least 100 million doses if their COVID vaccine got approval - which it did. As for Katalin Karikó, the formerly ignored proponent of mRNA technology, she is now Senior Vice President at BioNTech. The former "fringe" researcher certainly won't be short of a quid from now on. She's even been tipped as a potential candidate for the Nobel Prize of Medicine.
All this newfound wealth and talk of Nobel Prize nominations obfuscates a very discomforting reality. Namely, while the two key companies involved in mRNA technology - Moderna and BioNTech - have made shiploads of money, they have no previous track record in creating approved drugs, let alone creating drugs that have demonstrated long-term safety. Prior to the emergency approval of their hastily created and tested vaccines, the mRNA technology that their entire foundation was built on was problematic and displayed a penchant for triggering unwanted immune responses.
The mainstream bullshit factory is working overtime to obfuscate this reality. Many are insisting mRNA technology has been around for a "long time" with studies going back to the 1990s, neglecting to mention most of this research has been conducted in petri dishes and animals, and has proved highly problematic. Men's Health disingenuously writes: "In the past decade, there have been over twenty human clinical trials completed using mRNA vaccines. In recent years, mRNA vaccines have gained favor due to their ability to scale over traditional vaccine methods."
For some strange reason, Men's Health ignores the fact most mRNA vaccine trials were small Phase I and II trials and makes absolutely no mention that, before the COVID-19 panic, no mRNA drug or vaccine was licensed for use in humans.
But this same mRNA technology is now being feverishly rolled out around the world under the guise of "emergency use," and we are all expected to dutifully roll up our sleeves and take one in the ass arm.
You first, Men's Health.
So How Does this New mRNA Technology Work?
Cell biology is a complex topic, and a great way to make people's eyes glaze over. So I'll try and make this as simple and painless as possible.
Most people reading this would know that deoxyribonucleic acid (DNA) contains the genetic instructions for the development, function, growth and reproduction of all organisms, be it a tiny virus or the big, hairy, salty bags of flesh and bone known as Homo sapiens. Ribonucleic acid (RNA) is tasked with the job of coding, decoding, regulation and expression of genes. For want of a better analogy, think of DNA as the cell's CEO, and RNA as his group of personal aides that get stuff done.
There are many different types of RNA, but the one we're obviously concerned with here is messenger RNA (mRNA). The DNA in our cells use mRNA to convey genetic information that directs the production of specific proteins, including enzymes, hormones, growth factors, antibodies, etc, etc.
mRNA is created during the process of transcription, where a gene from the DNA is copied into mRNA. This information is then read by a ribosome (or a cluster of such known as polyribosomes) in the process of synthesizing a protein - kind of like construction workers examining an architect's instructions in order to work out where the the next bunch of steel beams is supposed to go. This process is known as translation.
The key point is that mRNA carry instructions and, theoretically, if you could artificially manipulate those instructions, you might be able to trick cells into creating specific proteins to achieve a certain desired physiological/biological outcome.
Which is the premise underpinning mRNA vaccines.
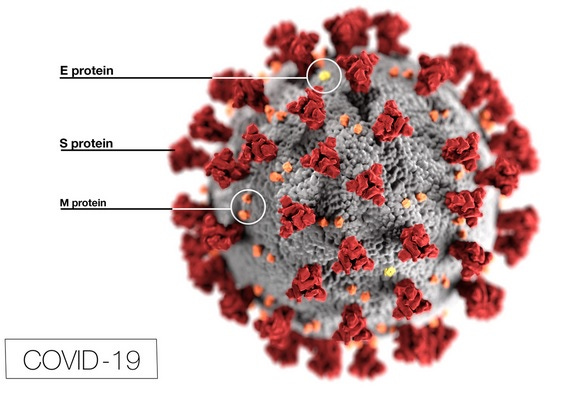
At the heart of the new vaccines is special mRNA that has been engineered to contain instructions on how to make a fragment of the “spike protein” unique to SARS-CoV-2 a.k.a COVID-19. The spike protein comprises those surface spikes you see in commonly depicted pictures of a COVID-19 virus molecule, like the one below.
This customized mRNA is given a special coating that will aid its entry into cells. In the case of the Pfizer/BioNTech and Moderna vaccines, this coating consists of liposomes and a chemical called polyethylene glycol (PEG). PEG has never been used before in an approved vaccine, but is found in many drugs that have triggered anaphylaxis — a potentially life-threatening reaction that can cause rashes, plummeting blood pressure, shortness of breath, and rapid heartbeat. So when severe allergy-like reactions occurred in at least eight people who received the Pfizer-BioNTech vaccine during a 2-week period in December 2020, many scientists naturally suspected PEG.
The NIH National Institute of Allergy and Infectious Diseases (NIAID, run by Fauci) was concerned enough to convene several meetings to discuss the allergic reactions with representatives of Pfizer and Moderna, independent scientists and physicians, and the Food and Drug Administration (FDA).
In other words, no-one's quite sure what is going on here. So when you see talking heads or read self-proclaimed experts belittling concerns over the unknown nature of mRNA technology, just remember they can't even work out what is happening with the mRNA coating itself, let alone the consequences of the actual modified mRNA.
But I digress. Back to our lab-modified, liposome and PEG-coated mRNA which is placed in a vial, then eventually extracted and injected into some trusting dolt's arm. The modified mRNA enters cells, where ribosomes read the instructions and assemble the requisite protein sequence.
Using the mRNA instructions, the cells create proteins that are structurally similar to SARS-CoV-2 antigens. These antigens then exit the cells and trigger the immune system to produce antibodies that recognize the spike protein on the SARS-CoV-2 virus. If and when COVID-19 infection does occur, these antibodies will hopefully mark the virus for destruction.
And so, rather than injecting a 'dead' or 'weakened' form of the virus into a person in the hope their immune system will create its own antigens, mRNA vaccines burrow their way into cells and directly implant a set of instructions to create SARS-CoV2 antigens.
mRNA have short lives - once their instructions have been read by ribosomes, they are broken down so their individual RNA nucleotides can be used again. Because mRNA vaccines have not undergone anything even resembling long term testing, it is currently unknown whether they offer lasting immunity against their targets.
The mRNA Vaccine Defenders: Using Red Herrings to Defend the Unknown
If you search around the internet, you'll find no shortage of blog posts defending mRNA vaccines by people claiming to be experts in cellular biology. These posts tend to follow a common formula: They "debunk" the claim made by some that mRNA vaccines will alter one's DNA, then declare the matter pretty much settled: The hysteria is overblown and mRNA vaccine skeptics are all a bunch of kooky conspiracy theorists.
It's not hard to see through the disingenuity of this strategy. Attacking one of the more fanciful claims made for mRNA vaccines, then portraying fears about their safety as unfounded, while ignoring far more realistic concerns, is just playing the old strawman game.
The real concern with mRNA vaccines is not that they will alter people's DNA and turn them into mindless, compliant zombies - the government, education system and mass media are already doing a great job of that. The real and very valid concern is that sticking a set of artificial instructions into human cells, using technology that has seen only brief experimental use in humans and has absolutely no long-term track record, could have unforeseen consequences.
If they were honest, the researchers championing this mRNA technology would acknowledge we know next to nothing of its long-term consequences. But they won't.

Some researchers, however, are a little more candid than their reality-evading peers. “There is a race to get the public vaccinated, so we are willing to take more risks,” Tal Brosh, head of the Infectious Disease Unit at Samson Assuta Ashdod Hospital, told The Jerusalem Post. Brosh acknowledged that there are "unique and unknown risks" to mRNA vaccines, including local and systemic inflammatory responses that could lead to autoimmune conditions.
Michal Linial, a professor of biological chemistry at the Hebrew University of Jerusalem, told the Post she believes there is no cause for concern. But when asked if she would take the vaccine right away, she responded: “I won’t be taking it immediately – probably not for at least the coming year. We have to wait and see whether it really works.”
A 2018 article by researchers from University of Pennsylvania and Duke Human Vaccine Institute, Duke University, also noted that autoimmune reactions were a possible risk from mRNA vaccines.
As it happened, we didn't have to wait long to learn of a very serious and unforeseen side effect associated with mRNA vaccine shots.
Pfizer-BioNTech COVID-19 Vaccine: "Safe, Effective" and ... Deadly, Apparently
All around the world, reports of deaths in people who recently received mRNA vaccines continue to mount.
On 16 January 2021, The Epoch Times revealed 55 people had died in the US after receiving COVID vaccines. In addition to the fatalities, there were 96 life-threatening events, 24 permanent disabilities, 225 hospitalizations, and 1,388 emergency room visits. The deaths occurred among people who received the Moderna and Pfizer-BioNTech vaccines, according to the federal Vaccine Adverse Event Reporting System (VAERS).
In Norway, 23 elderly people died shortly after receiving the Pfizer-BioNTech coronavirus vaccine. All reportedly died within a week of vaccination. More recent reports put the number at 33.
Neighbouring Denmark, Finland, Sweden and Iceland, have also reported post-vaccination deaths, says CBS News.
In Germany, 10 elderly people died within 4 days of receiving the Pfizer-BioNTech vaccine.
It's not just the elderly who are being struck down. In Portugal, a heartbroken dad is demanding answers after his daughter died two days after receiving the Pfizer-BioNTech vaccine. Health worker and mother-of-two Sonia Acevedo, 41, received the injection on December 30 and suffered a sudden death at home on New Year’s Day. Abilio Acevedo told daily newspaper Correio da Manha: "She was okay. She hadn’t had any health problems."
Then there's the case of Gregory Michael, a 56-year old Florida doctor who died just 16 days after receiving the first dose of the COVID vaccine on 18 December. The otherwise healthy Michael developed the rare blood disorder thrombocytopenia after receiving the vaccine, and died on 3 January after suffering a brain hemorrhage.
Pfizer said in a statement that it was aware of the death: "We are actively investigating this case, but we don't believe at this time that there is any direct connection to the vaccine." No, the pharmaceutical giants never believe their drugs have any "direct" conection to harmful side effects and deaths, even when the evidence is overwhelming, as the Vioxx fiasco lucidly demonstrated.
Michael's wife, Heidi Neckelmann, has no doubt his death was caused by the vaccine. "He was a very healthy 56-year-old" who "delivered hundreds of healthy babies and worked tirelessly through the pandemic," she said in a Facebook post. Michael was an avid tournament and big game fisherman as well as a rescue-certified scuba diver.
Ironically, Michael was a vaccine advocate, his wife said, before raising doubts about its safety.
Hypocrisy Bigger than a Hippo's Butt
In their thinly-veiled attempts to exculpate vaccines, authorities are demonstrating just how hopelessly hypocritical they really are.
The government of Norway, where 33 patients have died after receiving the vaccine, was one of the founders of the the vaccine shill group Coalition for Epidemic Preparedness Innovations (CEPI) in 2017, whose purported goal was to start preparing for a global pandemic. As its website states, "CEPI was founded in Davos by the governments of Norway and India, the Bill & Melinda Gates Foundation, the Wellcome Trust, and the World Economic Forum."
On 18 October 2019 – not long before COVID-19 mysteriously appeared out of nowhere - CEPI hosted an invitation-only pandemic simulation exercise at The Pierre Hotel in New York. The simulation was called “Event 201,” and magically predicted "an outbreak of a novel zoonotic coronavirus transmitted from bats to pigs to people that eventually becomes efficiently transmissible from person to person, leading to a severe pandemic. The pathogen and the disease it causes are modeled largely on SARS, but it is more transmissible in the community setting by people with mild symptoms."
Not surprising then, that the government of Norway is now trying to downplay the vaccine-related deaths, after initially acknowledging the drug may have been the culprit. On 15 January 2021, Dr. Sigurd Hortemo, chief physician at the Norwegian Medicines Agency, suggested side effects from the Pfizer-BioNTech coronavirus vaccine may have contributed to the deaths. He said in a statement that common side effects like fever and nausea shortly after vaccination may have led to more serious outcomes and deaths among elderly, frail patients.
"We cannot rule out that adverse reactions to the vaccine occurring within the first days following vaccination (such as fever and nausea) may contribute to more serious course and fatal outcome in patients with severe underlying disease," the agency said in the statement.
A few days later, the agency, who has been "working with" Pfizer on the matter, drastically changed its tune. It disingenuously claimed "no link" had been established between Pfizer-BioNTech's COVID-19 vaccine and any post-vaccination deaths in the country, even though the country had almost two dozen post-vaccination deaths linked to the Pfizer-BioNTech COVID-19 vaccine. Despite its dubious "no link" claim, it nevertheless recommended doctors consider the overall health of the most frail before giving them the shot.
"The reports suggest that common adverse reactions to mRNA vaccines, such as fever and nausea, may have contributed to worsening of their underlying diseases and a fatal outcome in some frail patients," the Norwegian Medicines Agency told CBS News. But it could not possibly have been the novel and poorly-tested vaccines that killed the patients. "The patients died from their underlying disease," insisted the NMA.
Of 13 cases analyzed so far, "they are people of advanced age, are frail and have serious illnesses, all of them," the director of the Norwegian Institute of Public Health, Camilla Stoltenberg, told reporters. "When it comes to causes there hasn't been any analysis done yet," she said.
Which begs the question: How can Norwegian authorities confidently declare the patients "died from their underlying disease" when no cause-of-death analysis has even been performed yet?
Here in Australia, where bald-faced hypocrisy is a prerequisite for public office, our bureaucrats are using similar irrational grounds to flippantly dismiss the vaccine-related deaths. Chief Medical Officer Professor Paul Kelly told the media, “In Norway in a normal week, 400 people do pass away in their aged care facilities. So this has to be put in the context of what has happened after people have received vaccines.” The vaccine rollout in Australia would continue unabated, he said.
And the shambolic Therapeutic Goods Administration (Australia's equivalent of the US FDA) said in a statement: "The deaths were recorded among very frail patients including some which were anticipated to only have weeks or months to live." Yes, just like the overwhelming majority of people who die with COVID are elderly incapacitated folks who probably only have weeks or months to live.
Federal Health Minister Greg Hunt said, "We don't know yet whether this is a function simply of age and people who are older and sadly facing the natural loss of their life, or whether there's any causation that hasn't been asserted as yet.” There was no evidence yet of a concrete link between the vaccine and the deaths, he claimed, and Australia's mass rollout of the Pfizer-BioNTech vaccine was going ahead.
You got that?
When frail, elderly nursing home residents in Australia with multiple other health conditions die after (allegedly) testing positive for COVID-19, authorities ascribe their death, not to their infirmity and multiple serious co-morbidities, but to their largely asymptomatic coronavirus. Not only that, but the rest of the country is forced into various states of house arrest and international travel is banned, effectively turning the former penal colony back into a prison island.
But when frail, elderly nursing home residents in Norway with multiple other health conditions die soon after receiving an incompletely-tested vaccine, authorities in both countries trip over themselves to exonerate the vaccine. There is "no link" between the new and poorly-tested drug from a serial lawbreaker like Pfizer and the deaths, they claim - it must have been the patients' underlying conditions, you see.
The idiocy reached giddying heights when Professor Kristine Macartney, director of the National Centre for Immunisation Research and Surveillance, said people should not be concerned about the reports from Norway. "We shouldn't at all be alarmed. We should just wait for the usual processes to occur, and any adjustments to clinical guidance or the product information will come if needed ... As vaccines are rolled out to millions, and ultimately billions of people across the world, we will see some flags pop up, but it's very important for people to understand that those will be really thoroughly investigated."
Oh, that's reassuring. If you drop dead after receiving the COVID vaccine, don't be alarmed, just wait for the usual bureaucratic processes of covering-up and excuse-making to occur, and everything will be just dandy.
Good heavens.
Of course, it's not just Australia and Norway where authorities are dialling up the shameless dishonesty. In the US, authorities insist COVID is so deadly that when a murder-suicide via firearm occurs, the cause of death is listed as COVID-19. Seriously. On 27 November 2020, police found Kristin and Lucais Reilly dead in their apartment in Fraser, in Colorado's Grand County. Their traumatic head injuries left little doubt as to the cause of death, and so the police pronounced it a murder-suicide. So too did the coroner pathologist. Based on evidence from the investigation and autopsy results, it was concluded Lucais shot Kristin before killing himself using a handgun he'd purchased in January.
But because the couple had reportedly tested positive for COVID-19 within 30 days of their deaths, the thoroughly dishonest Colorado Department of Public Health and Environment listed their causes of death as COVID-19.
You can't make this stuff up, folks. State and CDC reporting protocol requires that anyone who tests positive for COVID-19 within 30 days of their death be included in the COVID death count. As I have explained umpteen times, the US COVID death count is a complete fraud. As Anthony Fauci and Joanne Birx nonchalantly admitted back in April 2020, the US is counting anyone who tests positive - or is even suspected of being positive - as dying of COVID, even when the real cause of death was heart attack or kidney failure.
Meanwhile, the likes of Dr. Kelly Moore, associate director of the Immunization Action Coalition, said elderly deaths after a vaccine shot were "something we would expect, as a normal occurrence, because people die frequently in nursing homes.” He admitted on CNN that the COVID-19 vaccines have not been tested on the “frail elderly” and "we don't know how well the vaccine will work for them." Despite this, he insisted Americans shouldn't be too concerned by reports about the elderly dying “a day or two” after receiving the vaccine jab, adding such deaths are a “normal occurrence” that may have nothing to do with the vaccine since such people “die frequently.”
So get your head blown off with a gun, and the cause of death is COVID! But when an alarming pattern emerges of people dying shortly after receiving a new and poorly tested, poorly understood vaccine, there is no way it could have been the vaccine, no way, no sirree, scout's honour, that's a conspiracy theory, now move along, nothing to see here, we've got a nice cash cow going and we don't need you critical-thinking bastards to ruin it!
The Vaccine Research is a Farce
In order to quell any anxiety the frightened masses might have about the new Pfizer-BioNTech vaccine, pro-vaccine talking heads have insisted ad nauseum the drug has been studied thoroughly and proven to be safe and effective.
Nonsense.
As mentioned earlier, the Pfizer/BioNTech vaccine trial is still ongoing. It started on 29 April 2020, with estimated completion dates for primary outcomes of 30 July 2021, and secondary outcomes in September 2023.
The data that was used to prematurely rush this drug to market was taken from the first two months of the trial. To take data from a study that is less than one-tenth complete, use it to approve a drug, then claim that drug has been thoroughly and extensively tested is utter bullshit.
There are other issues with the trial, but before I discuss them, let's talk about the big brother of the Pfizer/BioNTech partnership. No matter which way you look at it, Pfizer - like all its multinational drug peers - is a corporate criminal. Between 2002 and 2010 alone, the company racked up $3 billion in criminal convictions, civil penalties and jury awards. The charges included cost report fraud, payment of kickbacks to physicians, fraudulent billing, and fraudulent marketing practices.
In 2012, US authorities charged Pfizer (and its subsidiary Wyeth) with paying millions of dollars in bribes to officials, doctors and healthcare professionals in Bulgaria, China, Croatia, Czech Republic, Italy, Kazakhstan, Russia, and Serbia during 2001-2007 in violation of the US Foreign Corrupt Practices Act. Pfizer subsidiary Pfizer HCP agreed to pay the Justice Department a $15 million penalty under a deferred prosecution agreement to resolve the investigation. Pfizer also paid the SEC $26.3 million in forgone profits, while Wyeth gave up $18.8 million in disgorged profits.
Pfizer, therefore, has a long and documented track record for dishonesty offenses. Anyone who willingly believe the claims of a company like that and is happy to take its hastily-approved vaccine must be a complete fool.
Seriously. If Pfizer was a person instead of a commercial enterprise that enjoys all the legal protections afforded to corporations, we'd call him a sleazy, corrupt, dishonest prick that deserves a very lengthy jail sentence. But because the world is run by corrupt assholes, Pfizer and its ilk are allowed to produce vaccines that politicians want to inject into every person on the planet. And because the average person is a clueless dipshit, many people are perfectly okay with this. In fact, a lot of them are literally crying out for this scenario.
But for those of you whose basic functions extend beyond eating, sleeping, shitting and nodding obediently at everything authorities tell you, any claims Pfizer makes for its drugs should be considered in the light of its well-documented history of criminal dishonesty.
So let's now turn our attention to the ongoing vaccine trial Pfizer is conducting with NASDAQ darling BioNTech. When pro-vaccine researchers, politicians, health authorities and bloggers tell you the vaccine is safe and everyone should roll up their sleeves and take one for the team, they're lying.
You cannot make such a claim from a trial which bears little relevance to real world conditions. The trial participants were clearly heavily screened during the recruitment phase, as supplementary data not included in the main paper reveal an unusually healthy patient sample.
Of the 37,706 trial participants for whom baseline comorbidity data was available, only 1.5% had suffered a heart attack or heart failure and only 1% had suffered a stroke. Only 3.7% had any kind of malignancy, 0.6% had mild liver disease (compared to the US average of 1.8%) and almost none had severe hepatic issues. The incidence of dementia was also so low that it was listed as 0%, while a piddling 0.7% had kidney disease (the prevalence of chronic kidney disease in the US is around 14%).
So the only trial for the Pfizer/BioNTech vaccine involves a fairly robust patient sample, and yet health authorities are allowing the vaccine to be given to frail, elderly people.
They are also failing to warn people with common health conditions like cardiovascular and kidney disease that they have been poorly represented in this trial.
To be eligible for the study, participants also had to be 16 years of age or older. You were not eligible for the study if you were pregnant or breastfeeding, immune-compromised or had any "Other medical or psychiatric condition including recent ... or active suicidal ideation/behavior or laboratory abnormality that may increase the risk of study participation or, in the investigator’s judgment, make the participant inappropriate for the study."
As such, the ongoing Pfizer/BioNTech trial is not equipped to inform us of the effect of the vaccine in those under 16, women who are pregnant or nursing, people with immune deficiencies and people with psychiatric issues.
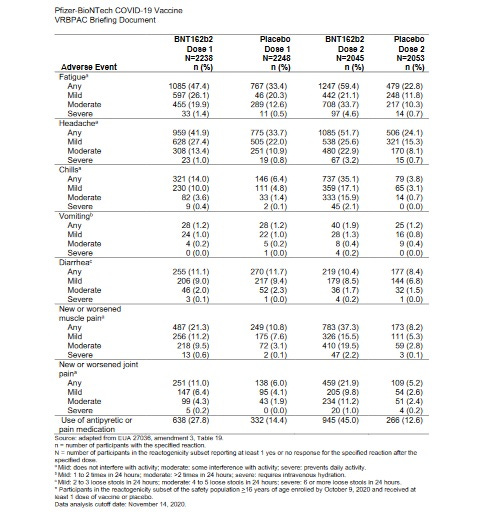
And even among the trial's highly-cleansed participant sample, the vaccine still showed a far higher rate of adverse effects than placebo. After receiving the second shot, 60% of the vaccine group experienced fatigue, compared to only 23% in the placebo group. Similarly, 59.2% of the vaccine group experienced muscle or joint pain, compared to only 13.4% of the placebo group. After the second shot, 45% of the vaccine group required pain medications, compared to only 12.6% of the placebo subjects.
As for the vaccine's highly touted 95% efficacy, the actual figures are a joke.
Of 18,198 subjects in the vaccine group, eight were diagnosed with COVID-19 during the first two months. Of the 18,325 placebo subjects, 162 were diagnosed with the virus. This where the "95% effective" figure you see splashed all over the media comes from. But if we look at the virus incidence in absolute terms, the COVID incidence figures are 0.04% and 0.88%, respectively. Not even a full percent in either group.
What a wank.
I'll also point out that if you were a shady entity - you know, the type that had racked up billions in fines for criminal dishonesty offenses - it wouldn't be at all difficult, in a trial with so many participants yet such a small number of endpoints being achieved, to manipulate the composition of the vaccine and placebo groups in order to increase the odds of getting a favourable result for your drug. Or you could simply pull a Study 329-style caper and alter the figures to your liking.
But of course, an upstanding corporate citizen like Pfizer would never do anything like that. Nah...
The ultimate point of all this vaccine tomfoolery, of course, is to stop the "deadly" COVID-19 virus. But there were no COVID-related deaths in either group. Two BNT162b2 recipients died (one from arteriosclerosis, one from cardiac arrest), as did four placebo recipients (one from hemorrhagic stroke, another from myocardial infarction and two from "unknown causes").
Wait a Minute...
On 10 December 2020, the FDA's Vaccines and Related Biological Products Advisory Committee met to discuss the Pfizer-BioNTech COVID-19 Vaccine. The briefing document is available here, and it contains some interesting figures not included in the main paper published in NEJM.
Scroll down to page 18 of the document, and you'll find a table with exclusion and dropout information. In any large clinical trial, you will inevitably have participants who drop out because their interest has waned, because they have moved, because they have developed concerns about being used as a "human guinea pig," and so on. A number of participants will also inevitably be removed from the study due to protocol violations, such as missing scheduled clinical visits or not taking or receiving the full treatment as instructed.
This is normal and to be expected.
What is not acceptable is when researchers exploit this phenomenon in order to skew the results in favour of their sponsor's/employer's drug. And make no mistake, this does happen. Take the notorious Study 329, one of GlaxoSmithKline's numerous misdeeds that, thanks to a whistleblower, came to the attention of New York Atttorney-General Eliot Spitzer in 2003. The GSK-sponsored study, led by Martin Keller of Brown University, brazenly omitted instances of suicidal behaviour in those taking the highly problematic SSRI antidepressant Paxil (paroxetine).
After two weeks on Paxil, a 14-year-old male participant punched some pictures, broke the glass, and cut himself badly. He was taken to the emergency room of a Fall River Hospital, but because he seemed acutely suicidal he was then transferred to Bradley Hospital, a psychiatric hospital for children and teens in East Providence. Despite the fact the boy was clearly suicidal and required hospitalization, he was not included among the listed patients suffering serious side effects in the published 2001 paper[1].
Another case uncovered by Spitzer’s office was a fifteen-year-old girl who entered the study in June 1995. In a memo to the institutional review board dated October 30, 1995, Keller wrote the teenager "was hospitalized on [September 15, 1995] due to becoming very combative with her mother and threatening suicide." But instead of coding her behaviour as an adverse effect, Keller said in his memo she was “terminated from the study for non-compliance.”
Another teenage girl was withdrawn from the study after deliberately overdosing on eighty-two Tylenol tablets. Again, instead of being listed among the subjects suffering adverse effects, she was described as having been ejected from the study for being "non-compliant"!
Like Pfizer and GSK, Eli Lilly is another serial offending corporate felon. Having lost its patent protection for its blockbuster Prozac in 2001, the company was eager for a new patentable antidepressant. The company's solution was Duloxetine which, just like its predecessor, promptly established a habit of increasing suicide risk. Lilly's solution to this inconvenient development was to to simply ignore as many suicides as possible.
In one of Eli Lilly’s studies, Traci Johnson, a healthy 19-year-old student who had taken duloxetine in order to help pay her college tuition, hanged herself. Her body was discovered on February 7, 2004, hanging by a scarf from a shower rod in an Indianapolis laboratory run by Eli Lilly. It turned out there was no record of Johnson and at least four other volunteers known to have committed suicide in FDA files, and Lilly admitted it never made public at least two of those deaths.
Pfizer itself has engaged in this sort of chicanery to protect the image of its popular antidepressant Zoloft (sertraline). Of sixteen sertraline trials submitted to clinicalstudyresults.org by Pfizer from the early 2000s, only 7 were published – and only 2 of those 7 studies reported on adverse events. The total number of "suicidal ideation, attempts, injury" reported in those two trials was 0. However, the summaries for the seven published trials retrieved from clinicalstudyresults.org in fact showed 5 instances of suicidal behaviour, and the summaries for the 9 unpublished studies showed a further 10.
Drug companies can and do manipulate study results in order to hide inconvenient findings and to make their lucrative drugs appear safer and more effective than what they really are.
Which makes the exclusion data for the Pfizer-BioNTech trial all the more concerning. Check out the following screenshot of the exclusion figures for the study.
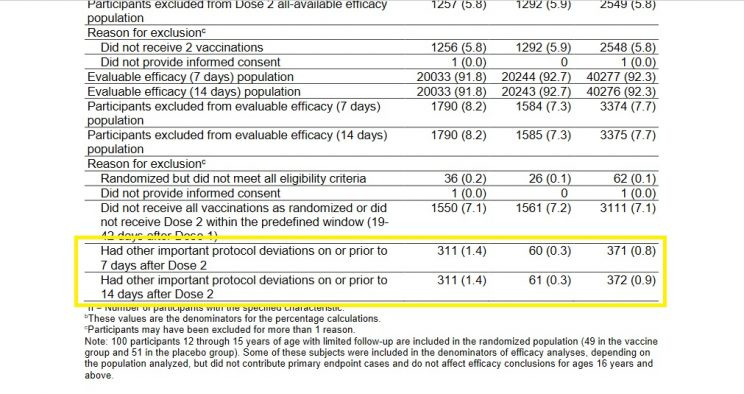
You'll note that a similar number of subjects were excluded from the study for not receiving all their vaccination/placebo shots - as one would expect in a randomized study.
But take a look at the figures for those excluded due to "other important protocol deviations," which I've highlighted. No specific reasons for exclusion are provided for the folks in this vague category, which makes it a great place for researchers to engage in some Study 329-style shiftiness. Cominarty recipients who experienced negative outcomes could easily have been "excluded" from the study, and hence the final efficacy and safety analyses.
Lo and behold, we see 311 subjects excluded from the study for unnamed "other important protocol deviations," but only 61 in the placebo group. No explanation, of course, is provided for this glaring difference.
When Peter Doshi, associate editor of BMJ, pointed out this highly suspicious anomaly, his critics countered that the 371 mysteriously withdrawn subjects in the Cominarty group comprised "less than 1% of the study population and can therefore hardly have influenced the study outcome."
Rubbish.
The 250-person difference between the drug and placebo groups dwarfed the total number of COVID cases recorded in the study. In a study with only 170 total COVID-19 diagnoses, and only 6 deaths, a 250-person difference in exclusions for no specific reason could have had a huge impact on the study's results!
The possibility of data-tampering is heightened by the fact that three Pfizer employees were tasked with the job of "reviewing all potential COVID-19 illness events." Even if these Pfizer employees really were blinded, it wouldn't be hard for them to nonetheless exclude subjects experiencing adverse events suggesting receipt of the Comirnaty drug (e.g., multi-inflammatory events). Unblinding would also have been facilitated by the fact that up to four times as many Comirnaty recipients received anti-inflammatory and pain medications.
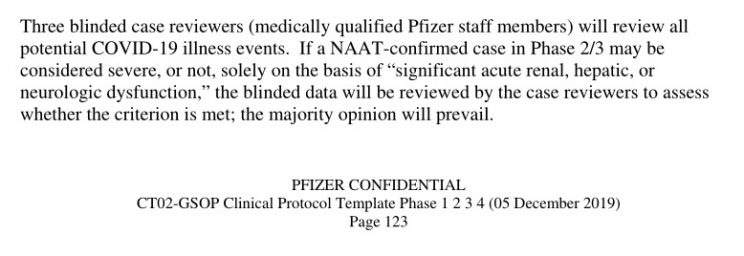
Offering up the full exclusion data for independent review would be one way of finding out what is going on here, but Pfizer isn't playing along. The data-sharing section in its trial protocol says "Pfizer will make available data from these trials 24 months after study completion."
Given that the study completion date is 27 January 2023, this means the data will not be released until 2025 - almost four years away! And even then, Pfizer will be very careful about who it releases the data to. As its data sharing section further states:
"Data requests are considered from qualified researchers with the appropriate competencies to perform the proposed analyses. Research teams must include a biostatistician."
Pfizer itself will decide who has the "appropriate competencies" to scour through its potentially embarrassing data. Only research "teams" with a presumably qualified biostatistician will be allowed to access the data, a stipulation that conveniently excludes capable but solo independent researchers from casting their critical eyes over the data.
Conclusion
Based on what has transpired so far, there is a possibility the Pfizer-BioNTech BNT162b2 vaccine will kill more people than it saves.
I'll give that a big miss.
I recently wrote about the potential for vitamin D to prevent and treat COVID, and discussed two small trials that found positive effects of vitamin D supplementation in COVID patients. After posting that article, kind readers alerted me to another Spanish trial that used the calcifediol form of vitamin D and also returned muy positivo results. This in turn led me to a host of other small trials that, when meta-analyzed, show a clear benefit to vitamin D supplementation against COVID-19. I'll discuss this all further in a coming article.
For now, I'll reiterate that what is unfolding with the Pfizer-BioNTech BNT162b2 vaccine seems to be a scenario we've all seen before, in which we are bombarded with overblown claims for a new drug, only for it to display unforeseen side effects.
Whether you wish to admit it or not, if you take any of the new mRNA vaccines then you are participating in an ongoing experiment, even though you never volunteered to be a research subject. You are placing your trust in drug companies, health authorities and politicians - all of whom have a long and documented history of spouting total bullshit - and becoming an unwitting vaccine guinea pig.
Good luck with that.
References
Bass A. Side Effects: A Prosecutor, a Whistleblower, and a Bestselling Antidepressant on Trial. Algonquin Books, Chapel Hill, NC, 2008 (Kindle Edition): 192-193.
The Mandatory “I Ain’t Your Mama, So Think For Yourself and Take Responsibility for Your Own Actions” Disclaimer: All content on this substack is provided for information and education purposes only. Individuals wishing to make changes to their dietary, lifestyle, exercise or medication regimens should do so in conjunction with a competent, knowledgeable and empathetic medical professional. Anyone who chooses to apply the information on this substack does so of their own volition and their own risk. The author/s accept no responsibility or liability whatsoever for any harm, real or imagined, from the use or dissemination of information contained on this substack. If these conditions are not agreeable to the reader, he/she is advised to leave this substack immediately.