



Mainstream Media and Biased Researchers are in Deep Denial About Mask Failure.
Masks don't prevent respiratory infections, but the mainstream will never admit it.

On January 30, the esteemed Cochrane Database of Systematic Reviews published a review of physical interventions to reduce the spread of influenzas. Most of the review was devoted to face masks, as these have been the most widely studied of such interventions.
I recently reported on the results here, but to quickly recap: The researchers reviewed the available clinical trial evidence and concluded that wearing medical/surgical or N95 masks"probably makes little or no difference” to your likelihood of getting a laboratory‐confirmed diagnosis of influenza/SARS‐CoV‐2.
When it comes to assessing the clinical evidence behind face masks, the Cochrane review is the most thorough and expansive published thus far.
However, the Cochrane review goes against the official mask narrative, and the mainstream isn't happy about it. As a result, globalist-controlled media outlets are either ignoring the findings or attempting to dismiss them on the most pathetic of grounds.
The Cochrane Database vs Regular Journals
Before I dismantle a couple of these attacks, a quick discussion of the Cochrane Database of Systematic Reviews is in order. The Database is part of the Cochrane Library, inspired by Scottish doctor and author Archibald Cochrane. A man after my own heart, Cochrane was critical of the lack of evidence behind many modern medical interventions and advocated the use of randomized control trials to make medicine more effective and efficient. Cochrane, wrote Shah and Chung in a 2009 tribute, "helped lay down much of the foundation for evidence-based medicine."
Two things set Cochrane reviews apart from the myriad of other systematic reviews and meta-analyses appearing in the published literature. One is their thoroughness; Cochrane reviews contain detailed information about the quality and methodology of each individual trial included in the review, something rarely seen in other published reviews.
The other standout feature of Cochrane reviews is that they are regularly updated. Realizing early on that a printed database would be outdated almost as soon as it was printed, the decision was made to publish electronically on CD-ROM (today, Cochrane reviews are available both online and on CD).
Repeated analyses have shown Cochrane reviews are consistently of equal or better quality than those published in print journals. A 1998 JAMA report found "Cochrane reviews appear to have greater methodological rigor and are more frequently updated than systematic reviews or meta-analyses published in paper-based journals."
A more recent analysis of cancer-related systematic reviews published in the Chochrane Database versus those published in high-impact medical journals found "Cochrane reviews were consistently of higher methodological quality, but cited less frequently."
Because they compare favourably against those published in big-name journals, Cochrane reviews are generally held in high regard. You can bet your bottom dollar that if the Cochrane Database found even modest efficacy for masks, the mainstream media would be shouting it from the rooftops.
But of course, that's not what happened.
Mainstream Media: A Bunch of Hopeless Mask 'Deniers'
I don't like the term "denier." At least not as it’s typically used nowadays. It's an ad hominem tag used by the left to snidely dismiss anyone who disagrees with them. If you highlight the many, many flaws in the anthropogenic global warming theory, you are branded a "climate denier." If you point out even a modicum of the infinite instances of corruption and absurdity inherent in the coronavirus con, you are labelled a "COVID denier."
But a "denier" is not someone who disagrees with you. It's someone who refuses to accept the reality of a situation.
And when it comes to masks, the mainstream are showing themselves to be deniers beyond compare.
The Whitewashington Post
Among those refusing to acknowledge reality is the Washington Post, the Bezos-owned bastion of hypocrisy that shamelessly runs the tagline "Democracy Dies in Darkness." That's incorrect: As the last 3 years have demonstrated, democracy dies in broad daylight, and corporate media outlets like the Post have been a major contributor to its demise.

On February 16, the Post ran an opinion piece by Leana S. Wen titled "Yet another study on masking causes confusion." The globalist force is strong with this one: Wen is a member of the Council on Foreign Relations, a global health fellow at the World Health Organization, a fellow for the U.S. Department of Defense and has served as a consultant to the Rockefeller-endowed China Medical Board.
She has also served as a consultant to the Brookings Institution, whose political leanings are not difficult to discern; it routinely directs over 99% of its political funding towards Democrats. Major funders of the $524 million 'non-profit' include the Bill & Melinda Gates Foundation, the $14 billion William and Flora Hewlett Foundation (a major funder of climate change activism and birth control outfits including Planned Parenthood), the far-left Hutchins Family Foundation (a major donor to the Democrats with intimate ties to the Clintons and the Obama Foundation), David Rubenstein (a billionare whose numerous appointments include co-chairman of The Carlyle Group, chairman of the Council on Foreign Relations and chairman of The Economic Club of Washington, D.C.), John L. Thornton (a former co-CEO and chairman of Goldman Sachs), JPMorgan Chase, the LEGO Foundation, the State of Qatar, the Government of Norway and the privacy-despising Australian Government.
Brookings accepted funding from Huawei from 2012 to 2018, and was named among over a dozen Washington groups to have received payments from foreign governments while encouraging American government officials to support policies aligned with those foreign governments' agendas.
Wen also served as president of Planned Parenthood, a eugenicist abortion-promoting outfit masquerading as a 'family planning' organization. Planned Parenthood performs over 380,000 abortions a year; based on figures from the pro-abortion Guttmacher Institute, that's over 40% of abortions in the US. To be fair to Wen, it appears she was not bloodthirsty enough for the infanticidal PP; she was kicked out in less than a year after having the temerity to place increased emphasis on non-abortion means of birth control.
Given her heavy left, globalist connections, it's not hard to guess where Wen stands on masking.
"First," says Wen, "I want to acknowledge that Cochrane is a highly reputable source. Its systematic reviews are considered the gold standard of medical analysis. But, as with all other research, any interpretation of its findings should take into account the methodology, the question being asked and the limitations."
Translated: "If the Cochrane review was supportive of masks, I'd cite it as a glowing, high-quality, eminently reputable scientific confirmation of face masking. But it didn't, so I am instead going to try and diminish its importance, and then cherry-pick from far lower quality evidence."
The bizarre argument Wen employs is that the Cochrane review only showed masking was ineffective at preventing "community transmission."
"Even if mask recommendations might not have a population effect," she writes, "high-quality masks still work on an individual level if that person consistently wears them."
Oh boy.
A community is nothing but a group of individual humans - often in close contact with each other. They work together, shop in the same spaces, sit next to each other on buses and trains, and walk past each other in often-crowded streets. If mask-wearing protects individual humans, then it should reduce virus transmission in the communities comprised of these individuals. One less person that becomes infected is one less potential "super-spreader," right?
I mean, what happened to the "wear a mask to protect others" bromide that was incessantly preached to us?
To support the utterly illogical "individual vs community" stance, Wen links to another opinion piece she wrote in February 4, 2022. In that article, Wen and her hand-picked 'experts' (i.e. people who parrot the party line) rely solely on a single uncontrolled study published by the terminally dishonest CDC.
That's right - from the dozens upon dozens of studies available, including controlled clinical trials - the best these folks can muster is a single serving of retrospective epidemiological slop.
That study can be found here, and the first thing to be noted is that it used the farcical test-negative design, the fraudulent nature of which I recently detailed here. The study recruited people who had already received a test result for 'SARS-CoV-2' during February 18 – December 1, 2021.
No actual health outcome - morbidity or mortality - was measured, or even mentioned. Testing for other influenza viruses also did not occur. The study measured nothing other than the likelihood of testing positive for "Sars-Cov-2" using the shady PCR test developed by the shady Corman-Drosten collaboration.
According to the researchers, "Always using a face mask or respirator in indoor public settings" was associated with 56% lower odds of testing positive for the Woohoo virus.
Among participants who specified the type of face covering they typically used, wearing N95 respirators was associated with an 83% reduced odds of testing positive for Sars-Cov-2, while surgical masks were associated with a 66% reduction.
Wen seizes upon these impressive-sounding figures, but barely touches upon the study's many shortcomings.
The first is that the aforementioned figures are relative risk reductions, and greatly exaggerate the true differences between groups. The actual absolute percent differences between groups were 6.9% and 9.3% for medical and N95 masks, respectively.
While far less spectacular than the misleading RR figures, they would still be worthwhile reductions if stemming from a randomized controlled trial - but they weren’t. They were obtained from totally uncontrolled junk epidemiology.
There were 1,828 participants in the study, but only 534 of them specified what type of mask they used - which tells us a lot about this study's quality and rigour (or, more precisely, lack of it).
To ascertain mask use, the study relied on self-reports and memory recall, leaving the results susceptible to faulty recall and social desirability bias (the tendency of survey respondents to answer questions in a manner that will be viewed favorably by others).
The researchers made no attempt to account for other preventive behaviors that could influence risk for acquiring infection. It is well-known that uncontrolled studies are prone to the "healthy user" and "healthy adherer" effect, where people who use one preventive measure are more likely to employ other preventive measures. The effect is so powerful that dubious interventions such as vegetarianism, low-fat diets and synthetic estrogen replacement (HRT) can actually appear beneficial because their users are more likely to engage in other truly healthful behaviours, such as exercise, temperate alcohol use, and smoking avoidance.
When these interventions are tested in randomized clinical trials and these confounders are removed, the mirage of benefit disappears. Just like it does for masks.
Which is exactly why we have randomized clinical trials, and why they are considered the gold standard for testing medical and health interventions.
But when this gold standard fails to produce the desired result for masks, Wen flippantly discards it and embraces uncontrolled, bias-prone junk science published by the CDC.
That's not good science - it's blatant denial.
The Conversation Has a Go at Flogging the Dead Mask Horse
Unlike Wen, leftist website The Conversation cited more than one study in its attempt to discredit the Cochrane mask review.
Like Wen, The Conversation is connected to all the wrong people - if you're after a non-partisan appraisal of anything related to COVID, that is.
Its "strategic partner" is none other than the Bill & Melinda Gates Foundation.
Its list of funders reads like a who's who of globalist mega-foundations and includes, among others: Alfred P Sloan Foundation, Andrew W. Mellon Foundation, Burroughs Wellcome Fund, Carnegie Corporation of New York, Ford Foundation, The Hearst Foundation, The Howard Hughes Medical Institute, Lilly Endowment Inc., Lumina Foundation, and the Walton Family Foundation.
So again, it's no surprise The Conversation is trying to diminish the recent Cochrane mask review.
The Conversaton's hit piece has already been soundly discredited by mask expert Megan Mansell. When I refer to Mansell as an expert, I don't mean she is a globalist-aligned researcher frequently quoted by globalist-aligned media outlets. I mean she is an OSHA-qualified PPE expert with an extensive background in the safe and effective application of masks in real-world settings.
Kicking a Bad Propaganda Piece When it’s Down
There are a few key pointers about the appalling Conversation article that I'd like to add and/or expound upon here.
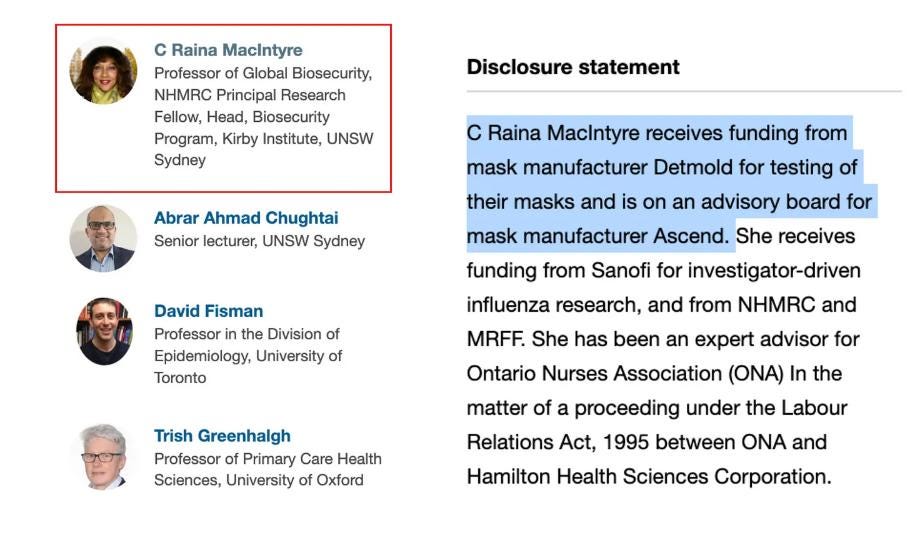
The first is that the lead author of The Conversation article is C Raina MacIntyre, a pro-mask researcher who has received funding from mask manufacturers Detmold and 3M (unlike MacIntyre, the Cochrane reviewers had no financial conflicts of interest to declare, and in fact have had to contend with politically-motivated pressure to water down their findings).

So again, it's a foregone conclusion as to what The Conversation article is going to claim.
Like Wen, MacIntyre et al begin their article by downplaying the importance of clinical trials. To believe Wen and MacIntyre et al, masks are a remarkably unique intervention that transcend the earthly bounds of RCTs.
Yeah, sure.
MacIntyre et al continue by throwing cloth and surgical masks under the bus. "COVID, along with influenza and many other respiratory diseases," they write, "is transmitted primarily through the air."
But, they continue, "(N95) respirators are designed for respiratory protection and cloth and surgical masks are not."
Take careful note that MacIntyre et al are stating in no uncertain terms that cloth and surgical masks - by far the most common in use - are not designed to provide respiratory protection.
Funnily enough, that didn’t stop her from claiming efficacy for cotton masks in a 2020 paper.
N95 masks, insist MacIntyre et al, are special. They are designed to fit closer to the face and block "95% or more of potential infectious particles."
Or so the theory goes.
♪ I Cite Myself, Ooh, I Don't Reference Anybody Else ♫
MacIntyre et al write:
"An RCT comparing occasional versus continuous use of respirators in health care workers showed N95 respirators and surgical masks were equally ineffective when only worn occasionally by hospital workers. They had to wear them all the time at work to be protected."
Oh, so now RCTs are suitable for examining the efficacy of masks?
Could this about-face have something to do with 3M and Detmold-funded MacIntyre being the lead author of that RCT?
MacIntyre et al complain in their Conversation piece that many N95 trials only compared the respirators to medical masks and did not feature a mask-free control group. Her solution, published in 2013, was to conduct a trial that only compared N95 respirators to medical masks and did not feature a mask-free control group.
Bloody brilliant.
That study involved 1,669 hospital-based health care workers in Beijing during the winter of 2009–2010. The participants were randomized by ward to three arms:
(1) medical masks at all times on shift;
(2) N95 respirators at all times on shift, and;
(3) targeted (intermittent) use of N95 respirators only while doing high-risk procedures or barrier.
The researchers state in their methods section that the study was conducted to measure the effect of mask type and use on five (5) primary outcomes (don’t get too hung up on all the individual types of bacteria and viruses; the key point here is that there were 5 endpoints):
1. Clinical respiratory illness, defined as two or more respiratory symptoms or one respiratory symptom and a systemic symptom;
2. Influenza-like illness, defined as fever (38°C) plus one respiratory symptom.
3. Laboratory-confirmed viral respiratory infection in symptomatic subjects, defined as detection of adenoviruses; human metapneumovirus; coronaviruses 229E/NL63 and OC43/HKU1; parainfluenza viruses 1, 2, and 3; influenza viruses A and B; respiratory syncytial viruses A and B; or rhinoviruses A/B by nucleic acid testing (NAT) using PCR testing.
4. Laboratory-confirmed influenza A or B in symptomatic subjects.
5. Laboratory-confirmed bacterial colonization in symptomatic subjects, defined as detection of Streptococcus pneumoniae, legionella, Bordetella pertussis, chlamydia, Mycoplasma pneumoniae, or Haemophilus influenzae type B by PCR testing.
Cost precluded testing all subjects, so only symptomatic subjects were tested.
MacIntyre et al triumphantly declared clinical respiratory illness was highest in the medical mask arm (17%), followed by the targeted N95 arm (11.8%), and lowest in the N95 arm (7.2%).
They also claimed "laboratory-confirmed bacterial colonization" was lower in the N95 subjects.
There were 5 endpoints, remember, but these are the only two outcomes that returned seemingly favourable results.
MacIntyre et al weren't so keen to point out that the rate of influenza-like illness did not differ between groups (0.7%, 0.4% and 1.0% in the medical mask, targeted N95 and N95-all-the-time groups, respectively).
Buried deep in the text, we also learn that "rates of laboratory-confirmed respiratory virus infections were low and not significant between arms."
We also learn the incidence of Influenza A or B 1 CRI did not differ between groups.
The lesson from this study is that N95 masks can be made to look effective by industry-funded researchers who carefully cherry-pick their outcomes, ignoring the more objective but non-supportive outcomes like laboratory-confirmed viral respiratory or influenza A or B infections.
These unfavourable results occurred despite a number of potential biases working in favour of the N95 group. The participants, of course, were not blinded and knew which group they were in. Participants wearing the supposedly superior N95 respirators all the time may have been more inclined to think they were enjoying superior protection, and hence more inclined to dismiss respiratory symptoms as a coincidence.
That's important, because only symptomatic subjects were subjected to lab testing.
The N95-all-the-time group reported a significantly higher habit of "hand washing after patient contact at all times." So this group may have been a more health-conscious group overall, which means other health habits could have influenced the results. Or perhaps the participants in this group - their identity being known to the pro-mask researchers - were given a few extra 'helpful hints' about personal hygiene that could have influenced their non-mask health habits?
On the topic of N95 masks, the Cochrane reviewers stated:
"N95/P2 respirators compared with medical/surgical masks may be effective for [influenza-like illness] ... (from 5 trials, 8407 participants; low-certainty evidence) ... (but) ... The use of a N95/P2 respirators compared to medical/surgical masks probably makes little or no difference for the objective and more precise outcome of laboratory-confirmed influenza infection" (Bold emphasis added).
Which closely aligns with what the MacIntyre et al study showed.
Cochrane review: 1
MacIntyre et al: 0
MacIntyre et al assert in their Conversation con piece that her 2013 study demonstrated that mask-wearing workers "had to wear them all the time at work to be protected." (Emphasis in original).
But their own data from that paper clearly show self-reported compliance was lowest in the N95-all-the-time group (only 57%, compared to 82% and 66% in the targeted N95 and medical mask arms, respectively).
Could that be the reason behind whatever paltry differences were noted?
Screwing Up the Natural Respiration Cycle is Good For You! Not.
Anyone who calls for mask use "all the time" during work shifts of eight hours or more is clearly so ignorant of the fundamentals of human respiration they should be instantly booted out of the health field, and instead made to go work in menial endeavours where they pose no danger to others.
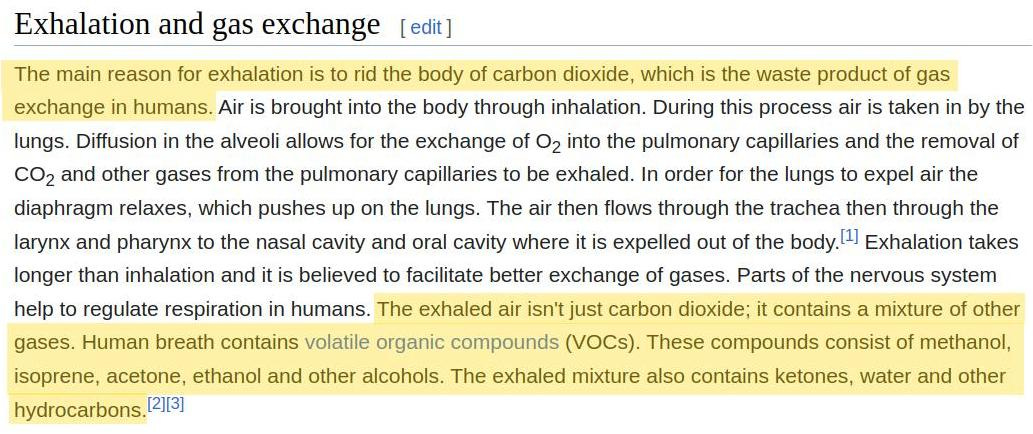
To repeat what we all learned in primary school science, humans exhale what is effectively "waste" air rich in CO2 and other gases, and breathe in fresher, more oxygen-replete air.
Even Big-Tech cancel culture behemoth Wikipedia admits:
"The main reason for exhalation is to rid the body of carbon dioxide, which is the waste product of gas exchange in humans."
When you don a mask, you introduce a very real physical impediment to the efficient removal of waste CO2 (and other waste products in breath). Here are some lucid visual demonstrations of what happens to CO2 levels in the air you exhale - and are forced to re-breathe - when you wear a mask.


Inverting the normal cycle of human respiration in this manner causes increased rebreathing of carbon dioxide (CO2) and a drop in blood oxygen saturation value. As the German researchers stated in a 2021 scientific review of mask side effects:
"According to the scientific data, mask wearers as a whole show a striking frequency of typical, measurable, physiological changes associated with masks."
By following the science, instead of government/media/biased researcher hogwash, we learn that masks reliably produce numerous side effects, including breathing difficulties, headaches, fatigue and exhaustion, increased chest complaints, uncomfortable temperature increases in skin and breath, dizziness, listlessness, impaired thinking, concentration problems, and increased pulse and heart rate.
There also the dermal complaints caused by masks, such as itching, rash, acne, and skin breakdown.
Based on these observations, confirmed time and again in controlled experiments and field studies, masks are not just a dumb idea for healthy humans, but an especially stupid idea for the elderly, pregnant women, people with skin conditions, those with cardiovascular and lung conditions, people engaged in exercise, those with neurological/psychiatric conditions such as epilepsy, dementia, paranoid schizophrenia, anxiety, claustrophobia and panic disorders.
While these effects are seen with all types of masks, 'superior' N95 respirators reliably produce a higher incidence of adverse outcomes.
Another group of German researchers analysed 46 patients presenting with rhinitis symptoms strongly associated with the use of FFP masks (the European equivalent of a N95 respirator). Nasal endoscopy showed nasal fluid accumulation significantly decreased after stopping mask use. The patients also subjectively reported decreased symptoms after 3 or more days after ditching their masks. Worryingly, the presence of polypropylene fibres isolated from nasal rinsing solution was significantly associated with the use of FFP masks in the patients. When you wear masks, not only are you inhaling unnantural and potentially pathological levels of CO2, you are ingesting synthetic fibres, the long-term health consequences of which are unknown.
All this, to prevent a re-branded flu with a survival rate of 99.73% …
It's beyond idiotic; the whole mask charade is like a collective, worldwide mental illness. When I see people driving along in cars, by themselves, windows up, and wearing a mask, I can't help but liken them to mentally ill folks who wander the streets screaming at imaginary enemies to leave them alone. Both are preoccupied with using ineffective measures to repel an enemy that exists primarily in their own fear-filled minds.
Mentally ill folks I can feel sorry for; people who flatly refuse to engage their own rational faculties to critically assess and dismiss the patently ridiculous, not so much.
Given there is not a skerrick of quality evidence to show masks prevent infectious respiratory disease, but plenty of evidence to show they reliably produce a plethora of unwanted side effects, their use as a preventive health measure is simply untenable.
But governments/media and biased researchers will never admit this, because they are hopelessly dishonest.
The way MacIntyre et al deal with this uncomfortable reality in their 2013 paper is to ignore it. They claim adverse effects were an additional endpoint, "measured using a semistructured questionnaire."
But nowhere do they share the results of this questionnaire. All we are told, again in a passage buried deep in the text, is that "in terms of comfort, 52% of the medical mask arm reported no problems, compared with 62% of the targeted arm and 38% of the N95 arm (P < 0.001)."
So 62% of the N95-all-the-time group did experience discomfort, compared to 48% and 38% of the medical mask and targeted arms, respectively.
But what were these discomfort events comprised of?
No answer.
Did the researchers care? Did they even bother to ask?
Again, no answer. No details of the sample questionnaire are provided; MacIntyre et al simply give a citation to a previous 2011 paper involving another mask trial they conducted. Retrieving that citation also fails to produce any sample questionnaire, but we do get a strong clue as to why the industry-funded MacIntyre was so reticent about reporting adverse effects in her 2013 paper. Here's Table 5 from that 2011 paper:
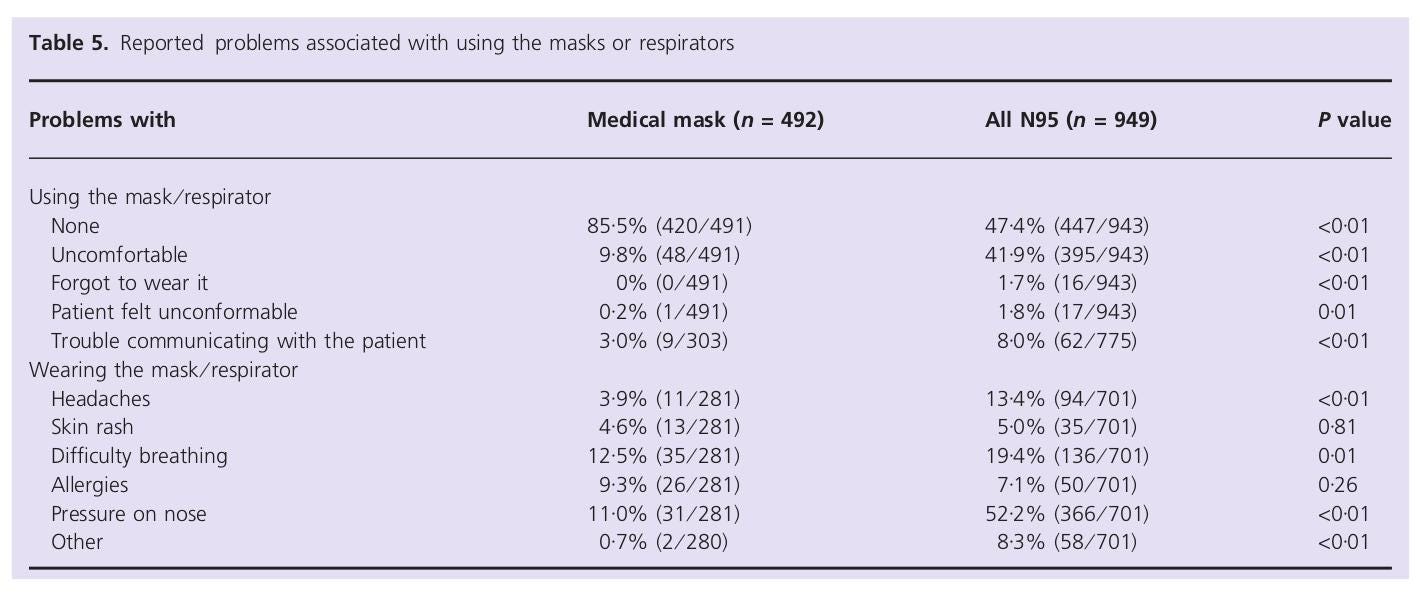
As the table clearly shows, wearing both medical and N95 masks were associated with numerous side effects. Worryingly, breathing difficulties and headaches were significantly more common when wearing N95 masks. The use of N95 masks also created more difficulties communicating with patients. I don't know about you, but if I was in hospital with a critical health condition, I'd damn well want to understand what the doctors and nurses were telling me. I'd also much prefer people about to make critical decisions about my health to be at the top of their cognitive game and not suffering headaches and breathing difficulties!
As the Cochrane review stated, mask harms in many trials were poorly and intermittently reported. When harms were reported, the reviewers noted, they were typically most frequent in the N95 groups. Which, again, is what we see in MacIntyre’s trials.
Cochrane review: 2
MacIntyre et al: 0
Apples versus Oranges versus Orange Apples, and Other Illogical Nonsense
MacIntyre et al's Onanist approach to science continues when they again reference themselves. This time, they claim to have compared "only apples and apples in a meta-analysis of two RCTs conducted in exactly the same way and measuring the same interventions and outcomes."
By comparing these "apples," MacIntyre et al claim to have "found N95 respirators provide significant protection against respiratory infections when surgical masks did not."
But when I click on the link they provide, the apples turn out to be a couple of rotten tomatoes. The two trials in their so-called 'meta-analysis' are the aforementioned 2011 and 2013 trials, both conducted in Beijing hospitals.
At this point, I'm tempted to roll my eyes, grunt "ugh!", and instruct readers to simply refer to everything I've written above and then multiply it by two.
However, it’s worth noting their 2011 paper included a mask-free control group. "The rates of all outcomes," claim MacIntyre et al, "were higher in the convenience no-mask group compared to the intervention arms."
But that control group was not randomized. Instead, this "convenience no-mask group," as the researchers described it, was selected from hospitals on the basis that most of their staff did not wear masks (apparently not the norm in Beijing hospitals), suggesting conditions in those hospitals were different than those in hospitals from the mask groups.
We'll never know for sure, because - in keeping with the low quality that seems to plague MacIntyre et al's 'research' - they presented no demographic baseline data whatsoever for the control group.
We do know, however, that the mask intervention arms were not equal groups. These intervention arms, listed in order of alleged efficacy, were medical masks, non-fitted N95 masks and fitted N95 masks.
But there was also marked difference, in the same direction, in the rate of high risk procedures each group engaged in (41% vs 35% vs 23.4% in the medical mask, non-fit N95 and fitted N95 groups, respectively).
So the N95 groups enjoyed the advantage of lower exposure to high risk procedures.
The fitted N95 group also had a significantly lower rate of influenza vaccination for the two winters prior to the study (conducted during China's 2008/2009 winter). While pro-vaxxxers will reflexively claim that as a disadvantage, the scandals and quality issues that have long plagued China's vaccine industry could in fact render this a big advantage.
Interestingly, the fitted N95 group also had the highest proportion of doctors, so the lower rate of vaccination in this group cannot be attributed to lack of education or lower socioeconomic status.
What this all means is that MacIntyre et al's so-called “apples versus apples” 'meta-analysis' was really just another proverbial comparison of apples to oranges!
Did I ever mention what an utter clown show modern science has become?
Oh, and for those of you who recoil in horror at the thought of hospitals without mask-wearing workers, MacIntyre note in their 2011 paper "we monitored all hospitals involved in the study for outbreaks which may have increased apparent attack rates, and none were documented."
Stop It, Or You’ll Go Blind
Ignoring the many trials examining mask use, and instead focusing solely on two that just happened to be conducted by yourself is a rather narcissistic approach to science.
Instead of limiting the N95 discussion to their own poor quality research, MacIntyre et al could've mentioned a 2019 paper reporting on a trial funded by the US CDC, Veterans Health Administration, and the Biodefense Advanced Research and Development Agency.
But they didn't.
To be fair, the CDC doesn't mention it either, and a look at the results quickly explains why.
Like the MacIntyre et al trials, the participant groups were randomly assigned to wear N95 respirators or medical masks (there was no mask-free control group). The study involved outpatient health care personnel at medical centers around the US.
In contrast to the MacIntyre et al trials, the medical mask and N95 groups in the US trial were evenly matched in terms of baseline characteristics. Both groups were of similar average age, ethnic mix, health and vaccination status, and occupational risk.
The results?
The incidence of laboratory-confirmed influenza infection events was 8.2% in the N95 respirator group and 7.2% in the medical mask group.
Regarding secondary outcomes, there were no differences in acute respiratory illness events, laboratory-detected respiratory infection events, laboratory-confirmed respiratory illness events, or influenza-like illness events.
Among the 68.8% of participants who provided compliance information, adherence was similar in the two groups; "always or sometimes" was reported 89.4% of the time in the N95 respirator group and 90.2% of the time in the medical mask group.
As the researchers concluded: "Among outpatient HCP, N95 respirators vs medical masks as worn by participants in this trial resulted in no significant difference in the incidence of laboratory-confirmed influenza."
Earnest Researchers vs Biased Researchers
There are two key types of researchers in the world: Impartial and agenda-driven.
Impartial researchers respect the scientific method, and form their conclusions based on where the science takes them.
Agenda-driven researchers don't follow the science, but instead begin with a preconceived conclusion. That conclusion is determined by their personal beliefs and/or who pays their bills. Agenda-driven researchers then distort the 'science' to fit their preconceived agenda. They belittle higher quality research that is not supportive of their agenda, while exalting lower quality research that supports it.
I think it's fair to surmise that MacIntyre et al are agenda-driven researchers. Just how badly is evinced by their reference to the most appalling mask study in the entire history of humankind, the disgraceful, oligarch-funded farce known as the Bangladesh Mask Study.
The Bangladesh Farce
This is where MacIntyre et al completely destroy their last remaining shred of credibility. They claim:
"A large RCT in the community in Bangladesh found face masks reduced the risk of infection by 11% overall and 35% in people over 60 years."
Well, that's what the oligarch-funded researchers claimed, but in reality the trial showed no such thing.
I have written at length (here and here) what an atrocious, hopelessly-biased espectáculo de mierda the Bangladesh trial was.
Among the more than 340,000 participants, over a period of 8 weeks, there was a difference of only 20 people testing positive for 'Sars-Cov-2'!
That pathetic figure was revealed by Ben Recht, Professor in the Department of Electrical Engineering and Computer Sciences at the University of California, Berkeley, after extensive sleuthing.
The Bangladesh researchers wouldn't share this figure in their preprint and Science papers, even though the primary endpoint of the study was whether masks reduced the number of individuals reporting "COVID-like symptoms" and testing seropositive for Sars-Cov-2 during the trial!
Instead, they only supply the highly misleading relative risk reduction percentages (I've addressed the RR ruse here).
That's not the only thing they're hiding from us.
On page 9 of their pre-trial protocol, the researchers stated that the outcomes would include:
"Hospitalizations and mortality (in both the village-level and individual-level experiments)"
Overall mortality is important in any intervention study that runs long enough for someone to die. In a study examining interventions for Sars-Cov-2/COVID, overall mortality is by far the most important outcome of all, because:
1. The entire premise behind turning Planet Earth into Planet Locked-Down-and-Completely-F**ked-Up was that COVID-19 was allegedly deadly like no other virus that ever came before it;
2. Overall mortality is the outcome least susceptible to fudging by researchers. You can sneakily re-categorize causes of death, but overall mortality is overall mortality - if a patient is dead, they're dead.
Which begs the question: Why was overall mortality - in fact, mortality data of any sort - missing from the published Bangladesh trial results?
I think we all know the answer to that question by now, but let's see what happened when Steve Agresti, President of Just Facts, emailed the study's lead author Jason Abaluck and co-author Ahmed Mushfiq Mobarak to find out.
On Oct 15, 2021, Agresti emailed the Yale duo and asked why the preprint claimed “mortality data was not available” (p. 86). As Agresti noted in his query, "This outcome is typically simple and straightforward to measure."
Mobarak's reply the next day fell neatly into the category of "ridiculous." He wrote:
"Mortality is a very rare outcome. If you are trying to detect statistically precise changes in rare outcomes you would need to do a population level RCT (collecting data from 600 communities would not be large enough), or study changes in policies at the country level and then rely on administrative data on mortality. Getting administrative data on mortality in rural Bangladesh in real time is not easy."
Mobarak has quite the sense of humour. Either that, or he assumed Agresti was stupid.
Mortality is a rare outcome? People die every day, but between November 2020 to April 2021, among 340,000 residents of a third world country, we're supposed to believe no-one died?
I mean, seriously?
Remember, this was smack bang in the middle of the "pandemic," when media reports would have us believe people were dropping like flies from the Woohoo virus.
So Agresti wrote back the same day, stressing the importance of mortality data and asking if the researchers would share whatever mortality data they did collect.
He received a reply the following day, this time from Abaluck, who claimed:
"Collecting mortality data would have required us to revisit every household at endline in order to survey them (we only collected blood from the small subset of households symptomatic during our study period). Given the nationwide lockdown that went into effect, another round of revisits would have been prohibitively expensive and complicated, and we prioritized the other outcome variables where we had much better hope of being statistically powered."
That, quite frankly, is an intelligence-insulting load of rubbish.
From page 17 of the pre-print:
"We began with 342,126 individuals at baseline. We were able to collect follow-up symptom data (whether symptomatic or not) from 335,382 (98%)."
So the researchers were able to obtain often highly subjective information about "COVID" symptoms for 98% of the study participants, yet the unmistakable symptom of death was too difficult to ascertain?
Modesty forbids me from stating just what I really think of that whopper.
Agresti wasn't buying it either. He replied:
"Given that your team was 'able to collect follow-up symptom data' from '98%' of the individuals in the study, why would they need to 'revisit every household at endline to survey them'? It seems like the bulk of this surveying was already done, and all that was needed is to follow through on the remaining 2%."
Agresti again asked for whatever mortality data the researchers might have had. "Did you collect mortality data during any part of the study before the endline? If so, would you share it?"
Tellingly, there was no response from either Abaluck or Mobarak.
Nine days after his unanswered email, he tried again.
That email has also gone unanswered.
The full email exchange can be viewed here.
Given that mortality was an explicitly stated endpoint in their pre-trial protocol, and that mortality data could easily have been collected at the same time as symptom data, I cannot come to any conclusion other than Abaluck and Mobarak are hiding the mortality data from the Bangladesh trial.
Furthermore, I can only assume the reason they are hiding that data is because it will reveal some unflattering truths about masks. Truths that they and their globalist sponsors - (whom, as I outlined here, includes all the usual suspects: George Soros' Open Society Foundations, the Bill & Melinda Gates Foundation, the heavily-left Omidyar Network, the Ford Foundation, and a myriad of United Nations agencies) - would prefer we did not know.
That's my conclusion, and it won't change until Abaluck and Mobarak stop proffering idiotic explanations to cover their evasiveness, and start exhibiting some transparency.
Sane people: 3
MacIntyre et al: -10
Conclusion
Masks might work against dust (the original target of N95 masks), but there exists no quality evidence whatsoever to show they prevent respiratory infections or infectious illnesses.
Use of face masks, however, does produce a very real risk of suffering from numerous unwanted side effects.
Anyone who tells you otherwise is a hopeless denier.
The Mandatory “I Ain’t Your Mama, So Think For Yourself and Take Responsibility for Your Own Actions” Disclaimer: All content is provided for information and education purposes only. Individuals wishing to make changes to their dietary, lifestyle, exercise or medication regimens should do so in conjunction with a competent, knowledgeable and empathetic medical professional. Anyone who chooses to apply the information on this substack does so of their own volition and their own risk. The author/s accept no responsibility or liability whatsoever for any harm, real or imagined, from the use or dissemination of information contained on this substack. If these conditions are not agreeable to the reader, he/she is advised to leave this substack immediately.